Volunteers and Local Healthwatch
One of the biggest challenges for local Healthwatch is how to best mobilise the many members of the public who want to contribute to improving local health and wellbeing systems.
who want to contribute to improving local health and wellbeing systems.
The challenge that Local Healthwatch faces is how to do this in a way that makes a system level impact. In this they are no different to LINKs and face the same pitfalls – the main one being to focus almost exclusively on recruiting their own volunteers.
I think that the LINK model put a great deal of emphasis on three types of voluntary engagement these were:
- A board of volunteers
- A team of volunteers providing services – information, office, enter and view etc
- A wider membership – who were comparatively inactive.
I do know that some local LINKs also engaged and worked with other organisations who also recruited and worked with volunteers and also with user led groups (patient and carer groups) which were run by people with a specific condition.
My impression was that for many local LINKs their energies focussed on supporting a comparatively small and dedicated group of volunteers – which took their energy away from wider system level ambition.
For Healthwatch to be powerful it has to locate itself within a wider context of volunteering at place level and its actions then stem from this understanding of context.
I have been messing around thinking about how to describe this context and have come up with this strange looking diagram – “the knickerbocker glory of volunteering ”.

The diagram suggests that there are 3 ways of considering volunteering with regard to Healthwatch which are connected and have different degrees of importance.
These are
- Healthwatch Volunteers;
- Health System ‘Voice’ Volunteers – where giving opinions or advocating is a key part of the role;
- General volunteers in the Health System who are providing services of different sorts – such as WRVS or people who provide luncheon clubs.
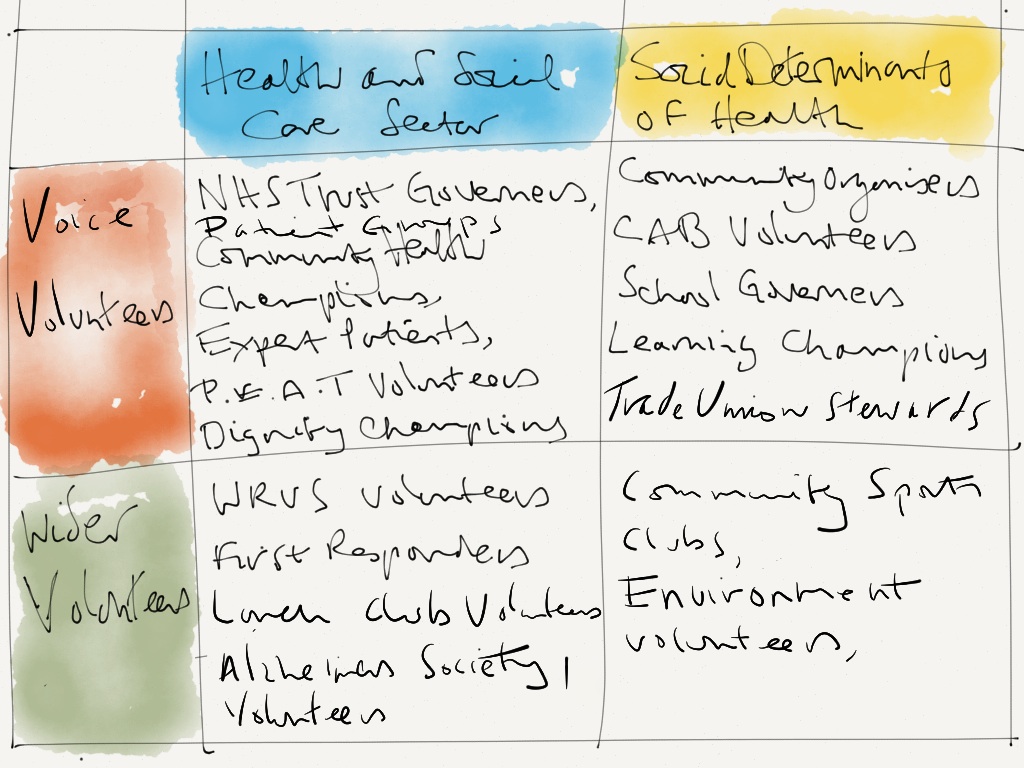
Running parallel to this ‘Health System’ strand are similar groups of volunteers who are also concerned with voice – such as school governers, welfare rights volunteers, trade unionists etc and a similar much wider group of volunteers involved in everything from culture through to environment. This group is of course equally important because health is not just about health and social care. The Social Determinants are equally important and these voice volunteers will be interested in a health and wellbeing too.
Here is a table showing the sort of volunteers that I am talking about (N.B. PLACE assessors are people who use a health service including current patients, their family and visitors, carers, patient advocates or NHS patient council members. PLACE stands for Patient Led Assessments of the Care Environment) Bear in mind that the volunteer roles in the table below are just examples – there are many more!
Obviously, its not possible to be connected directly with all of the volunteers described here. My argument is that a powerful Healthwatch will as a minimum have a strategic approach to being connected with all organisations who recruit, support and train ‘Voice Volunteers’ whether they are in the Health System or not.
What do you think?

Mark, your assessment of the LINk volunteers is very accurate, many times we were concerned about ensuring a qulity volunteer experience but this was very time consuming. The approach you suggest is perhaps a more sensible and productive way forward
Hi Mark, this is really helpful, thanks for sharing (lovely diagrams too). I’ve had ideas which I think run on a parallel with what you’ve pinned down here – I hadn’t jumped to a connect with Healthwatch volunteers. When I worked with a colleague from the (then) PCT a year ago to run a participatory session which encouraged thinking about what a local Healthwatch would mean for different community and patient based groups I encouraged participants to consider the stake which local sports clubs and friends of parks groups, for example, had in relation to health and wellbeing. I pointed out that they weren’t on the mailing lists for existing health fora etc., they often care passionately about improving health and work hard to do just that, and yet rarely engage in conversations with commissioners of health services … and so on.
Over the last few weeks I have been thinking about the activities which hundreds of local community groups plan and deliver on a completely voluntary basis which probably contribute significantly to the priorities in Dudley’s new Joint Health & Wellbeing Strategy. I think it’s unlikely that the work of such groups will be taken in to account in outcomes framework monitoring and thus their contribution overlooked. I’m already looking at ways that local sports clubs can connect meaningfully with the sorts of things that are in the JSNA and local strategies around health, and your post has helped me to think about this from another perspective.
Your thinking will definitely shape a discussion I have planned with a colleague from Healthwatch Dudley around volunteering and engagement. Thanks 🙂
Thanks Lorna – I appreciate your comments. Agree with you completely with regard to volunteers involved in local sports sports clubs, dance groups (I am a fan of Park Run – does this happen in Dudley?) etc – I think that JSNAs and associated strategies have too often led to the commissioning of new NHS led activities and failed to build on and support existing activity – and as you say also not capitalised on the experience and interest of the people who are providing these. It will be interesting to know how you get on with your ideas. Best wishes – Mark