Public Health England – Evidence into Action – I am not convinced
Reading the Public Heath England report ‘Evidence into Action” I sometimes get the feeling that Duncan Selbie is being held in a room by the Governments Public Health Minister and a bunch of doctors from the Health Protection Agency.
Every so often he manages to get out a passing reference to inequality or the social determinants of health – but for most of the time all that escapes the room is talk of diseases, clinical interventions and changing the behaviour of the irresponsible public.
The values are right.
“Evidence into Action” starts by recognising the importance of a new approach:
- that encourages everyone to gain more control of their health
- where prevention and early intervention are the norm
- where action on health inequalities is across all the wider determinants of health
- where assets of individuals families and communities are built on to support improved health
Unfortunately aside from a passing reference to “Due North” which is in effect the unofficial Public Health England Strategy (it has a very strong focus on the social determinants of health) the report rapidly defaults to a clinical view of priorities with the majority of the document focussing on 7 very traditional public health areas with predominantly technocratic solutions that fail to recognise the socio-economic circumstances that people live in.
These traditional areas are:
- Obesity
- Smoking
- Drinking
- Best Start in Life
- Dementia
- Anti-Microbial Resistance
- Tuberculosis
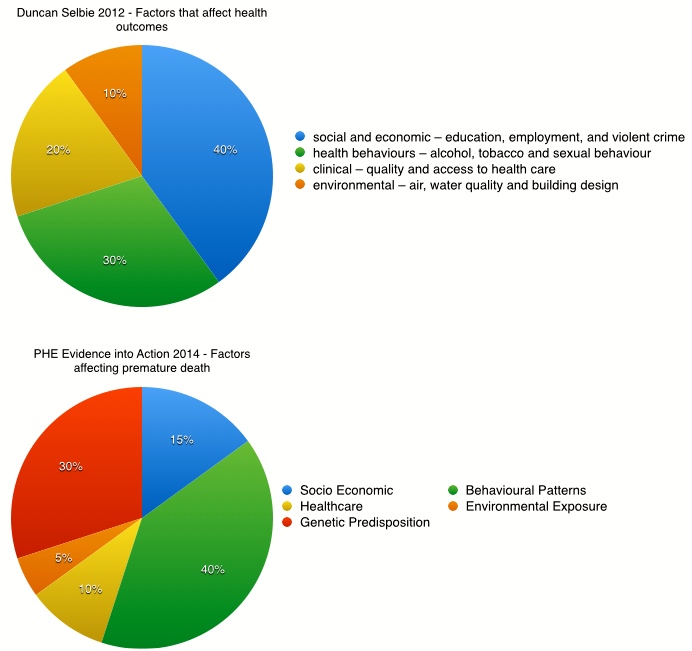
The rot sets in on page 6 with a graph which; while making the case that health care makes only a small contribution to preventing premature death also implies that the biggest contribution to premature death is behaviour. This contrasts with information that PHE was sharing in 2012 (Spotlight on wellness) when Duncan Selbie was clear that the biggest factors that affects the health outcomes were socio-economic.
This is important because while the rhetoric is about tackling inequality and partnership with citizens the priorities and actions are predominantly all about medical conditions and interventions that fall into one of three categories – treatment, legislation and behaviour change. This approach ignores peoples socio-economic circumstances and reduces citizens to consumers of services or even worse those whose behaviour needs to be changed.
This very traditional approach to breaking people into chunks of conditions or behaviours and then trying to treat these has two effects. It takes away the focus on the whole person and it does not see the socioeconomic context within which people live their lives.
Mental Health
Failing to take a holistic approach allows the focus on mental health to slip through the net (again). Mental Health is mentioned 7 times but always within the context of something else – obesity, smoking, work etc. This lack of attention means that the impact that chronic mental health problems have on people’s ability to take control of their own lives is not acknowledged and as importantly the effect of socio-economic conditions on mental health – debt, impact of welfare reforms, stress of exploitative employment (zero hours etc) is not heard.
Tuberculosis is a disease of poverty
A further example of the effect of failing to recognise the impact of socio-economic context comes in the section on tuberculosis. In fairness the report notes that TB disproportionately affects the most deprived communities. However it then sets out a set of actions that focus on structural change and clinical interventions. Nothing about poverty, decline in access to and quantity of housing, the growth of low wages and impermanent employment economies!
What is to be done?
I have now seen two public health ministers in their addresses at conferences say directly to Duncan Selbie – ‘we want Public Health England to challenge government policy – be a thorn in our side’. I think it is clear from this document that this is the last thing the government wants. The Department of Health clearly treats Public Health England as one of its dominions and has no intention of granting it even the limited freedom that NHS England ‘enjoys’.
Luckily there are those in Public Health England who are willing to support arms length initiatives – such as Due North which better reflect local priorities and reality on the ground.
What do you think?

I really liked your post. I think it says interesting things and true. Moreover, the public health is always on the narrow path between the political, technical and scientific knowledge. All these situations with large uncertainty margins. Sadly almost always ends up being the policy owner.
Reblogged this on UK Environmental Health Research Network.
I share Mark’s concerns: here’s a (slightly edited) letter I wrote to PHE the other day:
I was surprised recently when a colleague drew to my attention the PHE report ‘From evidence into action – opportunities to protect and improve the nation’s health’, with particular reference to the prominent Figure 1 and the data it shows from McGinnis et al – link below. As the following quote from that paper demonstrates, the data when presented in the paper are immediately followed by qualifications suggesting that their unqualified presentation in the PHE report is inappropriate and misleading, suggesting as they do that a very substantial proportion of premature mortality is attributable to individual behaviour. Following McGinnis’ phraseology, it would clearly be more sensible, cautious and scientific to combine the domains of environment, social circumstances and behaviour rather than to imply, as you do in the way you publish the figure, that behaviour is an independent variable.
(Quotation)
‘On a population basis, using the best available estimates, the impacts of various domains on early deaths in the United States distribute roughly as follows: genetic predispositions, about 30 percent; social circumstances, 15 percent; environmental exposures, 5 percent; behavioral patterns, 40 percent; and shortfalls in medical care, 10 percent. But more important than these proportions is the nature of the influences in play where the domains intersect. Ultimately, the health fate of each of us is determined by factors acting not mostly in isolation but by our experience where domains interconnect. Whether a gene is expressed can be determined by environmental exposures or behavioral patterns. The nature and consequences of behavioral choices are affected by our social circumstances.’
(From: J. Michael McGinnis, Pamela Williams-Russo and James R. Knickman. The Case For More Active Policy Attention To Health Promotion
http://content.healthaffairs.org/content/21/2/78.long )
Although there is reference in the PHE report to Due North, the priorities spelled out in the report relate primarily to lifestyle; and the influence of social circumstances – circumstances which have deteriorated substantially as a direct result of the public policies of the present government – are played down.
Best wishes, Alex
Excellent thought provoking analysis as usual – even if I’m looking at it 3 years later nothing much has changed! How did the proportion of influence on health for socio-economic factors fall by over 65% and environmental factors by 50% in just 2 years? It’s a remarkable achievement isn’t it? The serious point is that it is technically fallacious to view both lifetyle and socio-economic factors as independent variables
ignoring how the latter is a causal factor for many health behaviours – the ‘causes of the causes’.
This ‘Llifestyle drift’ is of course nothing new. Remember Liam Donaldson’s ‘Ten Tips for Better Health’ in 2001 – and the genius response from Prof David Gordon (‘1. Try not to be poor’ etc)? I suppose then the question is why does it happen and what can be done about it? It’s tempting to argue that moving the publc health profession into the Political sphere of Local Authorities and PHE has neutered it as an independent voice. But this would ignore the obsessive attention on behaviour that existed long before these changes. I think it has more to do with the profession’s self- perceived sphere of influence – focussing on what it believes it has the power to change (commissioning services) as opposed to what makes the biggest difference. In my view having a seat at senior levels of LA and Gov could and should help to reverse this ‘drift’ – using Health Inpact Assessment and a Health in All Policies approach has the potential to both influence policy makers and empower communities to advocate for real change. It is also the only solution to really address the tranformation needed to make health and social care systems truely sustainable. STPs anyone?
*