Road to Nowhere – PHE response to “Due North” Health Inequalities Report
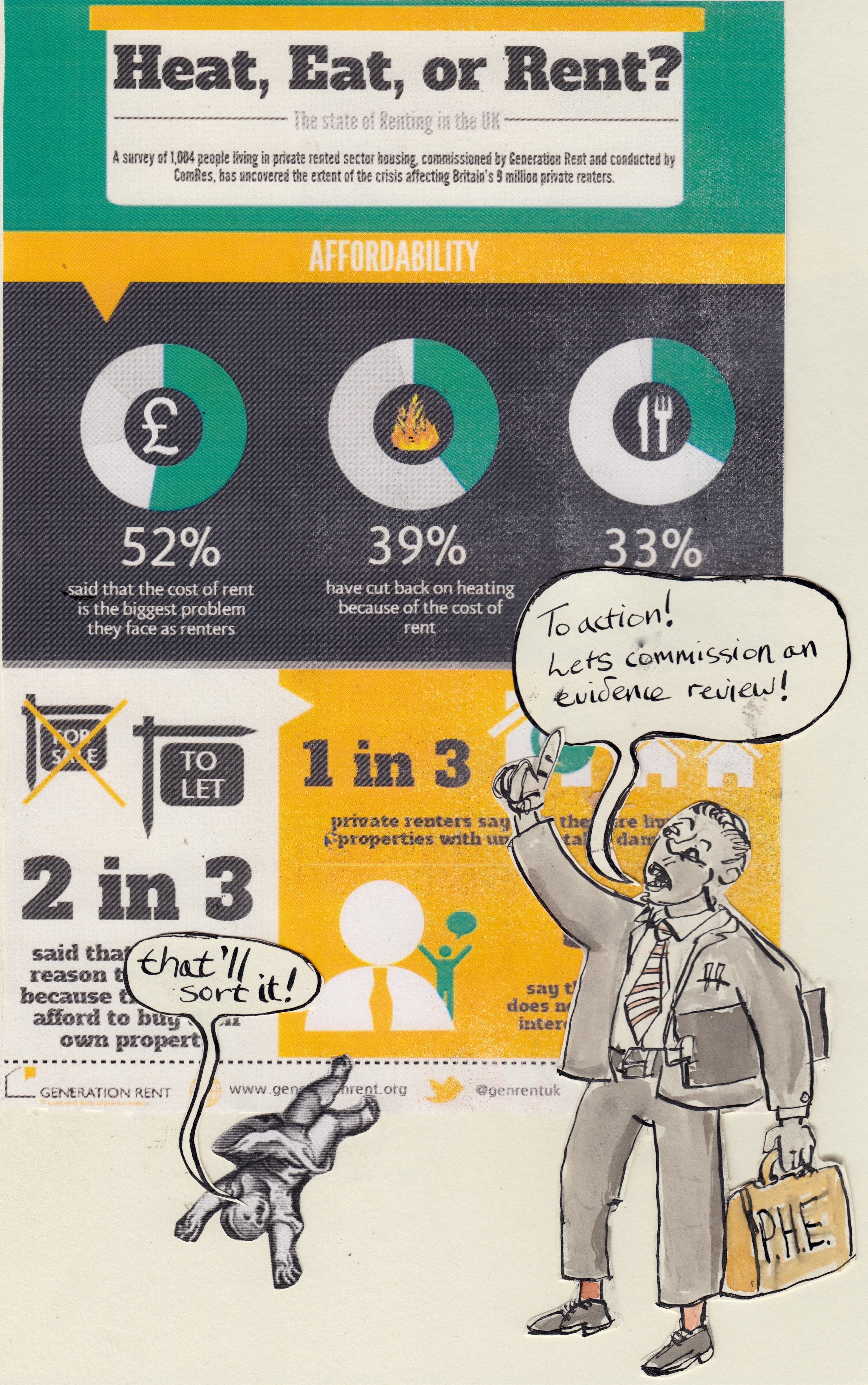
InfoGraphic by Generation Rent and Piktochart
The Due North report on Health Equity was published in September 2014 and in July 2015 Public Health England published their response.
When it was first published I shared my views on Due North on my blog here and here There were elements that I liked and others that felt to be important points but it was hard to work out what practical actions might stem from some of the challenges.
So I was keen to have a look at the 30 page PHE response – which when laid out on my dining room floor looks like quite e a long read!
Fig 1 – ‘the full monty’ – PHE Response to Due North 30pp
Luckily, once I had got rid of the case studies and contents pages it became a more manageable 10 pages – and I realised I could boot out the introduction as well which reduced it to a swift read before breakfast while the coffee was percolating.
Fig 2 – ‘the easy read’ – the actual PHE response to Due North 10pp

The two reports are a real contrast. The Due North report represents a coherent attempt by local authorities, the voluntary sector and academics to present an evidence based case for a stronger focus on the social determinants of health.
The Public Health England report is not a response to these recommendations – instead it is a statement listing work that Public Health England is already doing in related areas. There is one line in the introduction that refers to issues that have emerged from Due North specifically – mental health, violence and smoking – none of these are mentioned as possible areas of action for the future in the main body of the document.
Of course I know that Public Health England is an executive agency of the Department of Health – but I have attended two conferences where the Public Health Minister has said that they expect Public Health England to bring challenge to government policy. While I understand that this sort of public statement does not translate so easily into practice the latest Department of Health remit priorities letter for Public Health England states:
“The Government expects PHE to be an authoritative voice speaking for the public’s health and acknowledges that this can include constructive mutual challenge between PHE and national Government”
So, we should expect at least some public ‘challenge of national government’ Yet the PHE response does not appear to engage with the anxieties and concerns that local government has – for example the impact of welfare reform including the recent scandal over ESA deaths, cuts to local authority budgets, poor quality housing and the the role of the voluntary sector.
It talks about fostering debate but if this report is anything to go by it shows little evidence of ability to generate it.
Housing
Its actions feel anodyne, safe and irrelevant – for example its great that they now have an MOU with 20 agencies in the statutory and voluntary sector around housing and health. However, given that some of the real concerns are the present government’s policy commitment to push right to buy onto Housing Associations and the iniquitous role of a some private landlords where is the MOU with organisations advocating for tenants rights such as Generation Rent, Shelter and Citizens Advice? Where is the ‘debate’ about the health impact of further right to buy – given that there is now good evidence that the biggest single beneficiary of this policy are private landlords?
Voluntary Sector – How about getting a bit of a debate going now?
While the report indicates that PHE are part of the DH review into the future of the voluntary sector it could do better than say that they will wait until the outcome of the review – surely PHE has some view of the current role of and issues facing the voluntary and community sector and what it thinks might be some of the areas that are worth exploring further?
What to do?
Its clear that PHE are constrained by Government policy, I think the approach taken by Paul Johnstone in the North – commissioning an independent external agency like CLES is the way forward. I am not convinced that commissioning more evidence and producing more guidance is going to help a great deal.
Those of us at the grass roots need credible voices rooted in practice telling our stories and offering challenge at both a local and national level. So, we need more funding from PHE to independent agencies and to the voluntary sector who can genuinely generate debate and external challenge.
What do you think?

A very good exploration of the problem of our current public health structures. It is a tragedy that the Public Health Observatories have been abolished by PHE. One of their functions, amongst many valuable ones, was to generate hard hitting reports on serious public health issues. The sort of report that could not easily emerge from within a civil service body like DH or, currently, PHE. Public health needs to find its voice, but it is difficult to see where it will able to be secure enough to speak truth onto power.
I agree with Gabriel above, and admire his restrained voice. I am more cynical. Statements such as “The Government expects PHE to be an authoritative voice speaking for the public’s health and acknowledges that this can include constructive mutual challenge between PHE and national Government” come out of the Government’s PR handbook and should not be mistaken for actual guidance cf Sir Humphrey Appleby.
Mark thanks again for putting your ideas out there. I read your piece concurrently with Alex Scott Samuel and Katherine Smiths article on Fantasy paradigms of health inequalities which really affirmed to me that I can’t expect more from PHE as it forms part of that realm of “parrelell fantasy worlds” that construct responses to tackling deep issues that are easily manageable through downstream actions and focus (in terms of what to do and to whom) and therefore collude with the centralised Government policy focus, tone and rationale.
I reflect also the cargo cult (nicked that from Samuel and Smith) of the individual in all PHEs position – and his/her/their unhealthy behaviours and lifestyle – and wonder if they’d look more to communities, networks, place, power and agency as (one of) the real politics that the Govt needs reminding of?
It’s right you challenge PHE to speak truth to power more on the deep issues of social justice and health inequality and perhaps institutional / professional bodies need to be doing that too – and maybe there is a place for PH observatories or similar “local” bodies in doing that but I agree with a further point in Samuel and Smiths paper (p6) that there is a prevailing and institutionalised, normalised way of doing and being that conspires to filter out ideas and approaches about tackling for example health inequalities which don’t fit or concur with the established order of policy etc.
So what’s the way forward? Lobby via research, data? Promote action to enhance direct voice through local mechanisms that people are or can be involved in? Leave it to a particular professional lobby to agitate for PHE to do more on speaking truth to power – to paraphrase Lynne Friedli – that hasn’t worked in the past so why should it work now from the same professional platform.
Thanks.