Where are health Inequalities, Communities and the Voluntary Sector in the NHS England General Practice Forward View?

The General Practice Forward View is an important document, it sets out how NHS England proposes to support the development of general practice through to 2020/21. It is therefore important for all of those working in primary care and communities to understand the opportunities it presents and how it to access them.
Health Inequalities and Communities

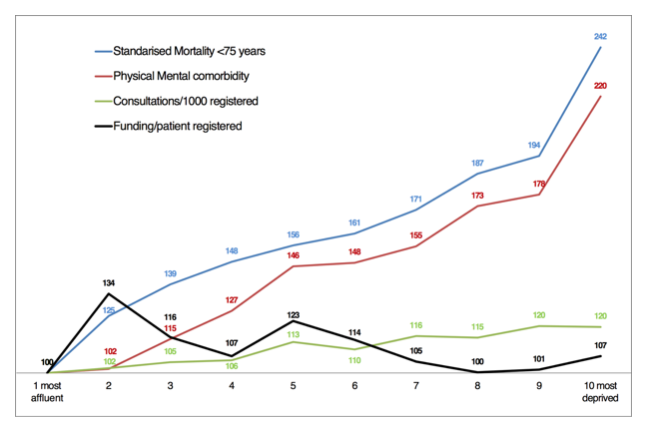
As the graph above shows it was disappointing to see that with the exception of social prescribing there appears to be little recognition given to the context within which General Practice works. So, there is little mention of inequalities and of deprivation and indeed of the voluntary sector.
This is concerning. In Sheffield we have started an exciting piece of work with practices who serve the poorest parts of the city. We recently invited Professor Graham Watt down from the Glasgow Deep End Group. Their work as is shown by the graph below (Scottish data) shows that practices serving the poorest communities are likely to receive less funding yet face much greater demands than practices serving wealthier areas.
Nonetheless the GP Forward View does present opportunities – not least because there are a range of commitments including one to revisit the GP funding formula to better reflect deprivation and rurality as well as a promise of more funding (£2.4bn more by 2020/1).
There are a number of levers for us to use – they include influencing the development of the Sustainability and Transformation Plans which will include £508m over the next five years to strengthen practice resilience (£56m), grow the medical and non medical workforce (£206m) and support practice redesign (£246m) and a development programme for practices (£30m). Similarly it will be important to ensure that CCG commissioning strategies for primary care include clear actions with regard to health inequalities and the role of the voluntary and community sector.
Here are three suggested actions.
- Data – any local authority/CCG area needs to be able to describe the particular challenge faced by practices serving the most deprived populations. The Glasgow Deep End Group focusses on the practices working in the 100 most deprived populations in Scotland. We need a similar hard edged focus. It is surprising difficult to re-create the graph above in a CCG area – but we need data on funding, health inequality and activity if we are to produce a robust evidence base that underpins actions.
- Service Models – It is the case that many GPs have developed hopeful productive working relationships with voluntary and community sector organisations. The current buzz word is Social Prescribing – but many of these relationships predate this. There is often a strong link to a neighbourhood organisation – or community anchor, many of these are members of Locality. This is important because service models and relationships will vary depending on the community. In Sheffield the recent neighbourhood based approach – People Keeping Well – based on populations of roughly 30,000 begins to recognise this level of organisation. Again, the CCG is currently undertaking a piece of work to capture different service models developed by 4 of these GP/Community Anchor partnerships. These service models should help us develop a more systematic approach to promoting ways of working that foster local partnerships with communities.
- Alliances – I know that this appears obvious. But in this case it is crucial to get General Practice staff, Active Citizens, VCS organisations and other allied services such as Pharmacy and Optometry to come together to design local service models. This is not just about consultations. This has to be an ongoing process of shared enquiry and requires different skills to the ones that NHS Commissioners have traditionally relied on. Again, we can learn from the Deep End model here who use a process of ongoing dialogue which continually spins off briefing papers and reviews. These have the potential to influence local strategies. The methodology is a bit similar to the Rapid Review approach that I referenced in an earlier blog.
What do you think?

I agree that this is very important work. The post-code lottery must show up starkly at the primary care level, and this sort of micro-analysis should be vital to any policy on health inequalities. Also agree with the three actions, but note that – as ever – the work that needs to go into building local alliances is considerable, usually unfunded/hard to prioritise, so that what goes on tends to be episodic and patchy.