NICE, Public Health and Local Government

Articles by Mike Kelly former Director of the Centre for Public Health at the National Institute for Clinical Excellence are always worth a read. He has just published one in the Journal of Public Health which looks at the role of evidence-based public health guidelines in local government.
One of the points that Mike makes is that councillors have a much broader view of evidence than the NICE model whose approach has its origins in evidence based medicine, peer reviewed literature etc. He notes that elected members must also take into account a range of other factors – such as their local knowledge and the views of their constituents.
Mike’s paper got me thinking – as he says – local authorities are democratic political decision making bodies and NHS organisations are not. As I explored this a bit further it seemed to me that NICE have pulled back from their public health function in the last few of years. I think Mike left NICE in 2014
NICE guidance is still mainly for the NHS. The NHS is essentially a collection of services – and despite various attempts to make it more accountable locally it is really an aggregation of different clinical health specialisms bound together by a post war policy commitment – these are managed by NHS England on behalf of the Department of Health.
Being a collection of services – the focus is on delivery. Respective governments have created a performance management system that focusses on individual service performance rather than their total impact on population health. NICE guidance works in this policy context.
In general NICE guidance focusses on one of 3 areas:
- technical practice with individuals,
- how services should work
- what systems should do.
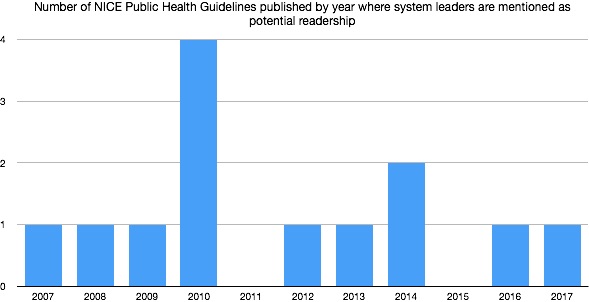
Most NICE guidance focusses on areas 1 and 2; however, NICE Public Health Guidance for understandable reasons has a greater focus on areas 2 and 3. Even here emphasis is more on services rather than systems. I have looked at the 65 NICE public health guidelines of these only 13 specifically mention that the intended readership includes system leaders such as elected members, Health and Wellbeing Boards, Local Strategic Partnerships etc. My working out is here.
Most NICE guidelines are operational and conservative. By this I mean they tell us what is already known. The aim is to ensure that good practice is used consistently. It’s not surprising that elected members are largely unaware of them – most are not aimed at them and those that include them are produced infrequently.
Local Councillors head up significant local democratic institutions who use their mandate to ensure that the interests of their population are served. They are responsible for shaping what it feels like to live in that area, the local authority power of wellbeing is a recognition of this.
Many are trying to improve health and reduce health inequalities in a world that doesn’t work according to the same rules as NICE guidelines.
It is quite understandable that local councillors have little interest in much of the guidance that is produced by NICE. Having said that I think that when it existed the Centre for Public Health at NICE must have recognised this problem because they produced a series of Local Government Briefings that attempt to speak to local authorities in their system role. While I think they still struggled with the operational nature of NICE evidence nonetheless they strike me as an attempt to reach out to system leaders like Councillors.
Unfortunately NICE is now pulling away from this innovation – see below:
Councillors are primarily concerned with strategic challenges which can include structural inequalities, access to employment, financial insecurity, social cohesion, health and care system integration etc.
Unfortunately these strategic public health issues are just not on the NICE agenda reasons include:
- The stronger the evidence the narrower the topic – NICE guidelines are more likely to focus on operational issues rather than strategic ones.
- The problems are strategic, complex and in the here and now – NICE guidelines are built on the past and the evidence base for primary preventions is weak -s ee UKPRP Rationale. Expertise from peers and faster moving think tanks like Happy City (Thriving Places Index) the LGA (The Power of Place – role of Health and Wellbeing Boards) and even the Health Development Agency feel more relevant.
- Some topics that worry local councillors just don’t get onto the NICE list of approved topics because its not a government priority.
(Caveat – this blog has been written over a few evenings – I’m not claiming that it is a full representation of all NICE work on Public Health. Declaration of interest I used to work for the Health Development Agency)
What do you think?

Interesting analysis Mark
I was wondering about the effect of the delegation of the Health & Social Care budget to City Regions as in Manchester – presumably this will lead to more local scrutiny, accountability and influence perhaps particularly on local PH issues? (Could be an extra incentive for us to get or act together on this side of the hill?)
Mike
Hi Mike – in theory the city region is an opportunity. Although as I understand it Manchester have included Health and Social Care in their delegated powers while in South Yorkshire our (shaky) city region model has stayed away from this. Some might say that the South Yorkshire and Bassetlaw Integrated Care System (formerly Accountable Care Partnership, formerly Sustainability and Transformation Plan) will do this – but this is an NHS initiative and the local democratic accountability is unlikely to follow unless local government engages with it and – in my view is able to take it over….see first point!
Thanks Mark
You said
“it seemed to me that NICE have pulled back from their public health function in the last few of years. ”
You are correct.
One of Lansley’s first acts when appointed as SoS Health in 2010 was to put a red pen through EVERY NICE guideline with an upstream public health component:
Click to access 186177
He preferred a “Responsibility Deal” partnering with multi-national corporations.
Their gain, our loss.
Do you agree that local government thus has a greater challenge when central government
a) sabotages guidance on the most powerful public health interventions
b) Cuts council grants by half
Best Wishes
Simon
Hi Simon – thanks for this comment – as you will have spotted I note that one of the problems is that all guideline topics have to be approved by central government. With regard to local government I think there is a problem when the agency responsible for gathering evidence is not able to acknowledge the political context that it is operating in. A range of other commentators – Greg Fell, Harry Rutter and David Hunter to name but a few – are also looking at this problematic area of evidence. I suppose my line is that NICE has ended up as being seen as the primary source of evidence – while it is actually only really good on operational technical stuff. This is not entirely the fault of NICE – we need to locate its offer appropriately in the wider environment of experience and evidence – recognising that the most useful strategic stuff – applicable to todays context will come from elsewhere – usually places that are independent of government like JRF, Resolution Foundation, IPPR, CLES, Centre for Welfare Reform etc.
All the best
Mark
I fully support the points made in your blog Mark.
I chaired the L G Reference Group set up by Mike Kelly to produce the L G Briefings and have experienced the journey you describe. Since MK’s departure resources allocated to PH by NICE (and dare I say it the interest) have reduced substantially.
I have made the point in recent years that the PH functions of NICE and the funding should go to PHE but government seem happy to stick with the old ‘NHS model’
Happy to help with further analysis if there is interest.
Thanks Phil thats a relief! Although I worked for NICE for 6 months when they took over the HDA I don’t have detailed knowledge – most of what I have put down is based on checking stuff out online – so it is a relief that the analysis feels right. It is interesting that you think that funding should shift to PHE. While I think that culturally they are closer to the policy world of local government than NICE. Their difficulty is that they are really a government department and lack the ability to bring public challenge. My inclination would be to shift the funding to the LGA to strengthen the work they already commission on public health. For example they commissioned Shared Intelligence to undertake the review of Health and Wellbeing Boards that I reference at the end of the piece. Best wishes – Mark
Hi Mark
You’ve reminded me of some of the comments I submitted during the Tailored Review of PHE in 2016 which also recognises that LGA has a role – relevant extract below.
Keep banging the drum!
“Now that a clear expectation for the delivery of public health improvement lies on the shoulders of local government it would seem equitable that the funding associated with the commissioning, development or production of public health quality standards and public health guidance, which will be key to ‘value for money’ considerations in future, should lie either within the direct sphere of responsibility of local government or with an organisation such as PHE which now has an established network of local government connections, an understanding of ‘front-line’ public health issues and a growing reputation for independent expertise.”
Thanks Phil – Its interesting to note that date of that review and your submission. It is a small point but I think that one of the issues is that the transfer of HDA functions to NICE happened before the Lansley Health and Social Care Act. In other words when the HDA went over to NICE in 2005 public health was still an NHS (PCT) function. Of course in 2013 Public Health went over to Local Government. I don’t think that NICE spotted the implications of this change at all with regard to culturally how they deliver guidelines to an organisation with a local democratic place shaping function. Looking at what you said it looks like you were aware of those implications!
This is an absolutely fascinating topic. Who *should* take responsibility for looking at the evidence of the interplay between how it feels to live somewhere and how healthy you are as a consequence. Although part of the picture, QALYs are quite a hard measure to achieve when considering, say, a library.
My point is, it’s a very complex area. Coalescing the best thinking and evidence is not straight forward – it’s multifactoral and looks at broader evidence-based metrics which may not be as ‘hard’ as some of those currently used by NICE. But, I can’t really identify another body with such a strong brand and reputation for looking at exactly this and getting the backing of the health sector for their findings. Indeed, perhaps if they were active in this space people would have a broader view of what keeps a society healthy that extends beyond ‘what we invest in health services’.
Thanks.
Thanks for this – I agree it is difficult. However, it is instructive to check out a good article on the importance of evidence in Health and Wellbeing Strategies that was in the recent Journal of Public Health (https://academic.oup.com/jpubhealth/article/40/suppl_1/i13/4925601) that shows the importance of locally generated evidence.