VIRTUAL WARDS – Will this increase in NHS capacity widen Inequalities?
The NHS Operational and Planning Guidance for 2022/3 sets out a significant target for the system level roll out of virtual wards.
Here is the target
“By December 2023 to have completed the comprehensive development of virtual wards towards a national ambition of 40-50 virtual beds per 100,000 population.”
According to my maths – England has a population of 56 million which equates to (560*45) the creation of a minimum of 25,200 virtual beds in England. According to the Kings Fund, England has experienced a significant decline in acute hospital beds and currently has just over 100,000.
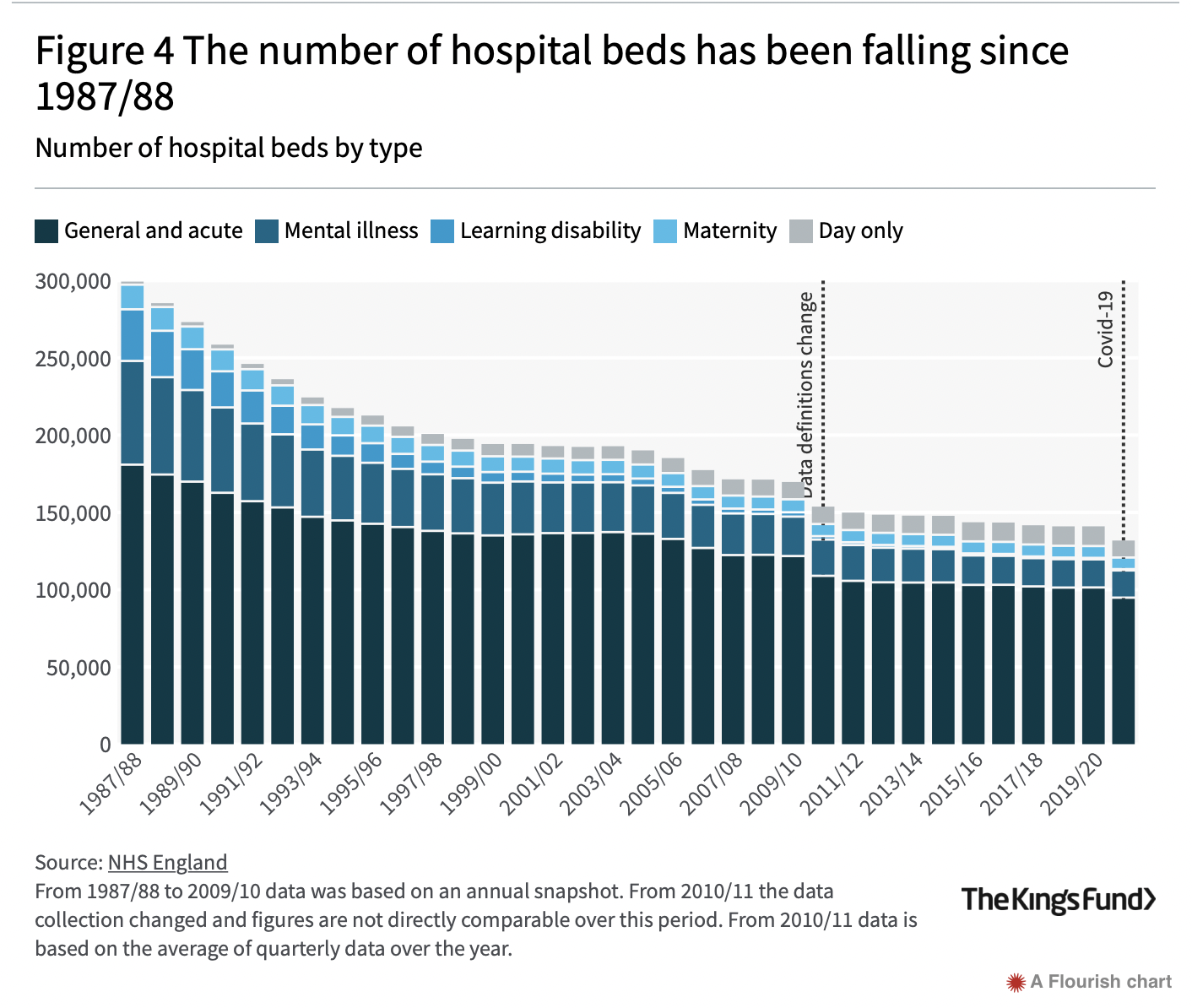
So this proposal equates to a 20% increase in beds – assuming that actual hospital beds are not reduced further.
Here is the money
NHSEI has allocated a total of £200m in 2022/3 and £250m in 2023/4 subject to targets being met (pp23/4 of operational planning guidance).
This £450m is transition funding only, and the second tranche of £250m has to be match funded by local systems in order to be released. This means that after 2023/4 local health systems will have to manage costs of running 20% plus beds from within their own resources.
The implementation costs equate to £450m/25200 = £17,900 per new virtual bed.
What is a virtual ward?
According to the NHS Supporting Information virtual wards:
“Support patients who would otherwise be in hospital to receive the acute care, remote monitoring they need in their own home or usual place of residence (I assume this means a care home).
..provide acute clinical care at home for a short duration (up to 14 days) as an alternative to care in hospital.
…are suitable for …. People with respiratory problems, COVID-19, heart failure or acute exacerbations of a frailty led condition”
What’s not to like?
I think there are two areas to be concerned about – which need more thought and action.
Inequality and Equality
The supporting information document I mention above is prefaced by a standard NHS statement – see below.
However the subsequent document makes no mention of why equality and inequality are relevant to this agenda and what actions might need to be taken with regard to the implementation of virtual wards.
Here are some suggestions:
The government has an ambition that 20% of acute beds will be provided at home in Communities. We know that:
- people with multi-morbidities are over represented in poorer areas
- Many people who experience health inequalities (core20plus5 group are more likely to live in poor quality housing, have low income and experience greater financial security
- The virtual ward model places a strong emphasis on digital connectivity -yet there is good evidence that disadvantaged communities lag behind with regard to access to digital technologies.
If we are to develop virtual wards in a way that does not widen inequality we need to consider how these will impact on people whose ‘virtual ward’ experience may be significantly worse than someone with a secure income, decent housing and good digital connectivity.
This leads me on to my second point…..
Integrated Health and Care systems
The current proposal feels like lifting and shifting a clinical model from a hospital to a community setting. Just because it is not in a hospital does not make it any more of a community based service – unless it is integrated into the local voluntary and community sector.
The ‘virtual ward’ patient is likely to require greater support from family or other carers, may require access to welfare rights and housing assessments etc. All of these can be addressed through a stronger funded connection with local voluntary organisations and local government etc.
What needs to happen
The NHS talks about the need to have a stronger focus on inequality and about shifting investment towards community and the voluntary sector, the virtual ward process needs to have:
- robust measures to understand the impact on inequalities
- have an explicit focus on capturing examples of good practice that address inequality and involve collaboration with the voluntary sector – this Leeds example looks interesting
- Costed plans to address the needs of patients living in poor conditions with fragile incomes
- Costed plans to ensure that the potential of the local formal and informal voluntary and community sector is utilised.
What do you think?

I have been listening to the early plans and scaling of this initiative, as chair of a mental health/learning disability Trust in a deprived area. My honest view is that the integration agenda helps, in that we will need hospital, community and primary care teams to share information, care, risk and Accountability to create hospital grade care in private dwellings. We’ve done a bit this winter.
However, to typify, the quality of housing stock, resources, connectivity and support varies massively from a deprived area to a well heeled home in a suburban setting. I’ve been out with community Midwives and nurses to do routine checks on new borns and community patients in deprived areas facing austerity and the contrast in working conditions is drastic. Its sometimes hard to gain access into gated community settings, or even locate a response from an isolated, probably often sleeping patient.
To launch and safely scale up Virtual Wards – which I emphasise, are a viable and evidence based option; people do recover very well at home in good conditions – needs protracted preparation, a carefully developed workforce and pathway, and a confident steps. Alternatively, trying a quick and cheap launch when hospitals are full, in a new austerity period, and depleted staff are barely holding on to key standards, will not go well. Clinicians will not be comfortable accepting hospital grade responsibility for a patient that is not fully under their care to a suitable level.
Thanks for the response Jeremy – a really thoughtful and balanced view as always – like you I do think that virtual wards do have the potential to make a significant contribution. We all learnt lessons during the pandemic about the added value of digital and phone to improving access. However, I do think that if we are to make the most of this transformation there needs to be a recognition that substantial investment is required alongside the Virtual Wards programme in local community and local government services.
This really thought provoking blog and certainly something those involved in developing virtual wards should give due regards too, as part of the scop. Wider determinants of health and care will certainly need to be considered to ensure the creation of virtual Wards does not widen the health inequalities gap.
Thanks Mark.
There are 2 ways health inequalities could be incorporated. I presume that as part of the assessment for a virtual ward, you would look at the patient IN CONTEXT of their environment. With poor housing or support a virtual ward is less likely to be an option?
The knock on effect of course is that, if you class virtual ward as superior to actual ward, this still exacerbates health inequalities. But it is safe.
Secondly if there is a social aspect to a virtual ward intervention, it’s possible that visits could have an element of assessment and engaging of services that could support the person more broadly. This often happens through the process of being in people’s homes. Something a real ward may never have chance to do.
Hi Ben thanks for reading and leaving the comments. I agree that as part of any assessment peoples lived context should be taken into account. I am a tad concerned with your point that action involves excluding those in poor housing and financial circumstances – the implication is that safety is something that is the prerogative of well off! However, this must not mean that people living in poor housing etc are excluded, rather Integrated Care Systems and acute hospitals should be working with PCNs, the local authority and the VCS to ensure when people are found whose living conditions are detrimental to their health that a joint approach is taken to addressing these. I think this will mean that the NHS will have to fund some of the activities required to address this. This will need to be costed into virtual ward development and revenue costs.
I agree with your second point – providing a virtual ward in the community will bring traditional acute care into the community with the benefits that that can bring. But, volunteering is not free – there are costs to organising volunteers (ask Paul Harvey!) and a new health service must be costed to recognise these. All the best – Mark