Public Involvement and the NHS – not good enough!
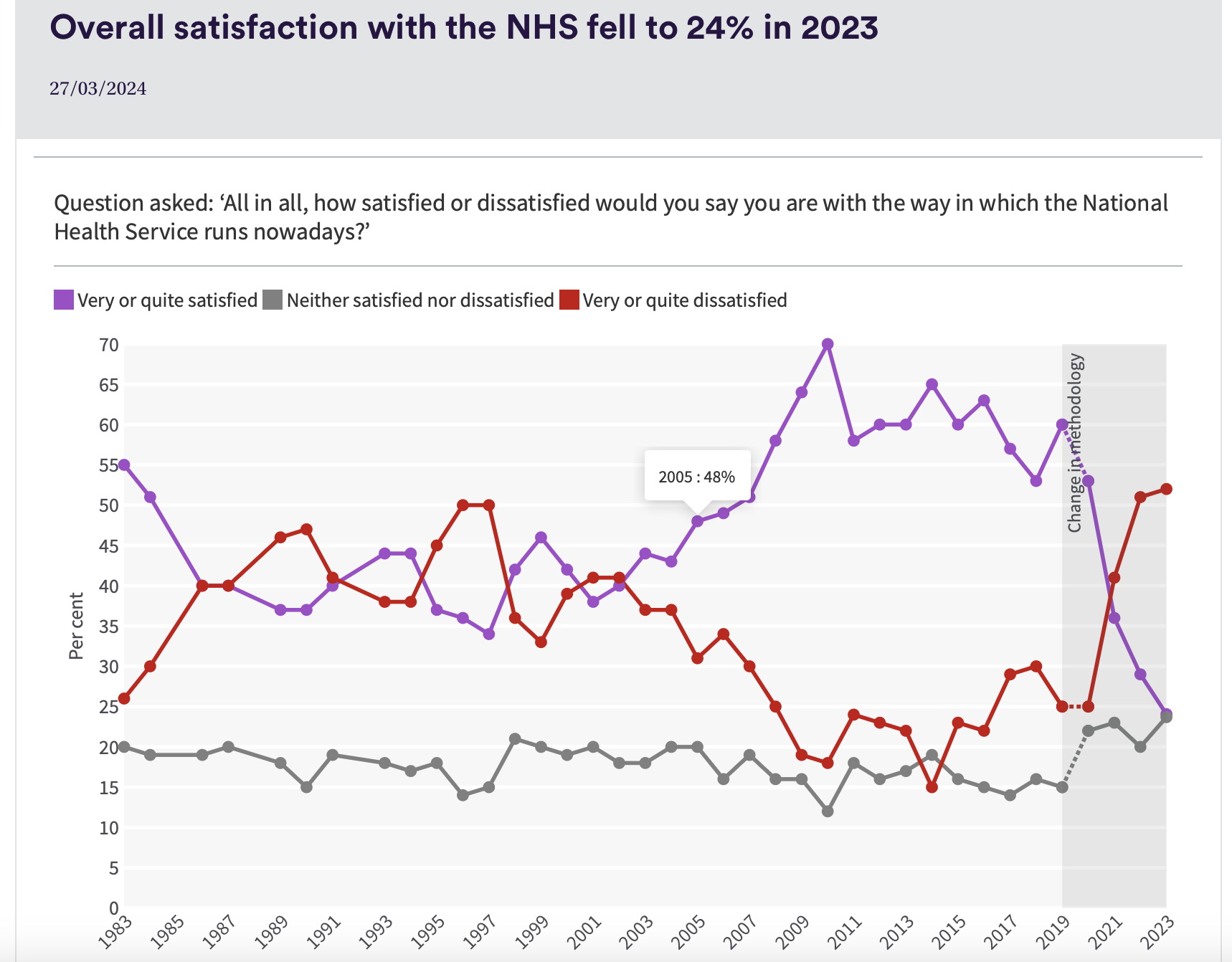
 Nuffield Trust Research published in 2023 survey shows the decline in trust in the NHS over time.
Nuffield Trust Research published in 2023 survey shows the decline in trust in the NHS over time.
As we start a period with a new government it has never been more important that local NHS services take meaningful system level action to develop stronger relationships with the public.
It is quite clear that we cannot rely on peoples automatic support – not least because large sections of the press and social media increasingly default to blaming health professionals and NHS management for the problems that the NHS faces. We need the public to be able to articulate what they would like to see in the NHS – at the moment we are too easily at the mercy of well intentioned but ill informed analysis – see below!

Public Involvement has always felt like a Cinderella activity in the NHS. In one way this is understandable – the purpose of the NHS is to deliver services to improve health – its purpose is NOT to provide public involvement.
Integrated Care Boards leadership
Integrated Care Boards are expected to produce a separate involvement strategy.
This requirement is spelled out in “Working in partnership with people and communities: Statutory guidance” published in 2022

I have had a look at the three strategies in Yorkshire and I am underwhelmed. The three ‘strategies’ are here.
Humber and North Yorkshire ICB
Concerns
Not accessible – they are all very long – it is ironic given that they are involvement strategies that they appear to have given little thought to who might want to read these. All seem to have sections that are cut and paste from the original statutory guidance – they read more as high level manuals on practice.
Lack of clarity – they don’t feel clear about what the role of the ICB is with regard to involvement. They have a tendency to default to how the public will be involved in the working of the ICB. There is insufficient recognition that the role of the ICB is to commission services in their area – and presumably this therefore means services that have strong accountable relationships with the public.
 No analysis – there is little or no analysis of the current state of play of involvement and engagement in each of the NHS organisations that they commission. There is also little clarity about practically what good should look like in terms of feedback and involvement in decision making structures. This means that champions for involvement in NHS organisations and outside such as Healthwatch are not given levers they can use to strengthen involvement.
No analysis – there is little or no analysis of the current state of play of involvement and engagement in each of the NHS organisations that they commission. There is also little clarity about practically what good should look like in terms of feedback and involvement in decision making structures. This means that champions for involvement in NHS organisations and outside such as Healthwatch are not given levers they can use to strengthen involvement.
Structures – None of the strategies describe how the ICB itself will change the way that it works to ensure that involvement and engagement is treated as a strategic priority going forward. This is important – a clear locus such as a committee responsible for involvement provides a place to organise, discuss and influence.
What good looks like
There are plenty of examples of good practice most of these are small scale and reliant on individuals.
I have mentioned some of these in blogs I have written in the past.
The include the work of the Birley Practice in Sheffield – using a Facebook group to develop stronger dialogue with patients about the service and to help patients understand what staff are trying to do.
The Peoples Voices Partnership in Leeds – originally established by Healtwatch Leeds and now part of the City’s Health and Care Partnership.
Care Opinion – which uses intelligent story telling software to give patient feedback and encourage dialogue. Frankly I find it staggering that none of the plans I read give a feeling for the degree of effectiveness of different patient feedback mechanisms by NHS organisations and their relative merits.
Going Forward
In my view this is urgent – leaders in Integrated Care Boards need to take a step change here – it is crucial to the future of the NHS going forward that ICB and their NHS organisations develop a strategic framework that meaningfully and comprehensively improves involvement with the public.
What do you think?
Tricky Times – tackling health inequalities in the NHS

Excelsior – with thanks to Henry Wadsworth Longfellow – haha!
Last year I wrote a blog which looked at how 3 Integrated Care Boards (ICB) had used ring fenced health inequalities funding. Following this the NHS Confederation asked me to undertake a wider review of a more representative sample – in the end this was 20 of the 42 ICB.
A team of us at Leeds Beckett University interviewed the Health Inequalities leads from each ICB.
Empathy with ICB
Health Inequalities is a wicked issue – it exists due to complex reasons to do with power, culture, prejudice and the economy. The situation is getting worse not better.
ICB have only been in existence for 2 years – so actions are not going to lead to a quick fix – so lets have some empathy for health inequalities leads in ICB. Their job was made harder when year two NHSE cut 30% of their management budget.
A strategic system level approach to address health inequalities is needed.
The funding we looked at was ring fenced in year one specifically to address health inequalities – and went into the baseline for subsequent years. £200m -sounds a lot – but it pales into insignificance against an NHS budget of some £168bn. The ICB have a duty to address health inequalities (highlighted in text here) – it should be the case that ALL NHS funding is stress tested to take account of its impact on reducing inequality not just the £200m. In our interviews some respondents were clear – this health inequalities funding is a catalyst to help them influence the spending of this much larger allocation.
It was clear given the time pressures particularly in year one that health inequalities leads tried to get the money out of the door before the end of the financial year in the most responsible way possible.
These decisions were made without an explicit overarching plan – the first Joint Forward Plan was only required to be produced by the end of the first financial year.
The real test going forward is whether this ‘catalyst’ funding model helped to bend NHS spend to reduce health inequalities more effectively – at this stage we just don’t know.
Third, Leadership is more important than ringfencing
Ringfencing really did not protect this funding. If a leader in the Integrated Care Board wanted to take the money to use it to pay off a deficit they could and in a number of cases did. We found that among half of our interviewees some or all of the money was used for purposes other than health inequalities. In some cases Health Inequalities leads never saw the funding at all – it was spent on deficits and never came to them.
More positively of course, half of ICB used the funding specifically to tackle health inequalities … so it is possible!
Cultural Change in ICB
Many ICB changed the governance architecture of the organisation – changing its culture through establishing high level accountable committees that usually reported to the Board. These involved wider stakeholders and were called things like population health and integration committees, health and equalities boards, population health management and health inequalities groups
NHSE still treats inequality as a second order issue
It was clear that the influence of NHSE is crucial here. Their top priorities remain things like hospitals performance in terms of finance, waiting times and service quality.
To paraphrase one respondent:
“We get must attend high level calls from NHSE holding us to account for our performance on topics waiting times or financial balance, we have never had a call from NHSE saying we want to speak to about your performance on reducing health inequalities”
This is not to denigrate the work of the NHSE National Healthcare Inequalities Improvement Programme led by Professor Bola Owolabi which was generally viewed positively by interviewees. Both for the development of the CORE20PLUS5 framework and for fighting for this catalytic funding.
Final thoughts
- Strong leadership in ICB is crucial to giving space to address inequalities
- Cultural Change such as changing the ICB Committee structure is essential to develop a shared analysis and action plan AND to empower ICB leaders take a different path to national priorities
- The real challenge is using the smaller health inequalities pot in a way that enables strategic change in the NHS system as a whole.
What do you think?
Its important! Arts, Community, Culture and Inequality.


This week Locality are launching the findings from a piece of research we (Leeds Beckett, Social Life and Locality) completed last year for the Arts and Humanities Research Council (AHRC). The AHRC were interested in research that looked at the relationship between access to the arts or environment, reducing health inequalities and the sustainability of this type of work.
Our research findings can be found on the Locality website here.
This research funding stream is linked to the National Centre for Creative Heath and is one of the actions that comes from the 2017 All Parliamentary Parliamentary Group Creative Health Report. This report subsequently influenced the development of the Arts Council England strategy – Lets Create.
There is clearly a growing recognition of the importance of creativity and health in improving health and wellbeing however, national strategies tend to focus primarily on the role of professional artists and creators and on the role of NHS Social Prescribing. While these are important these strategies tend to ignore the fact that it is community anchor organisations that build positive and trusted relationships with people – particularly people who live in areas of high health inequality, using access to creativity and the natural environment to do this.
Our research project ARCHES (Arts and Culture in Health Ecosystems) worked with four community anchor organisations to understand how and why they used access to the arts and the natural environment to build positive relationships with local people.
The four organisations we worked with were:
Halifax Opportunities Trust
ACCM
St Paul’s Trust
Pembroke House
All of these organisations provide a range of activities that build on peoples strengths and interests and create a positive place where people could feel good about themselves and build relationships with each other and the community anchor.
These activities included community gardens and allotments, cooking, oral history, writing, singing and dancing.
Some of these activities were led by arts and environment specialists. Sometimes they were employed by the community organisations and sometimes the community organisation provide the space and the relationships for the arts organisation.
What we learnt
- Community anchor organisations are embedded in these communities. They know that it is their responsibility to build and sustain long term meaningful relationships with the people who live alongside them.
- Good community anchors (of which there are many) understand and facilitate outside experts such as artists to bring their skills to communities, they are not in competition with arts or environmental organisations. They provide a gateway and foundation that arts and environmental organisations can build on.
- Policy makers and commissioners (in arts and health) do not sufficiently understand the important role that community anchors play. They are a key part of the delivery chain – building trust and relationships and through this enabling people to engage with activities that build on their ambitions and strengths.
- Through these relationships community anchors help people to connect with other services which are specific to issues that concern them – these can be as diverse as welfare rights or cancer screening.
- Finally, commissioners such as the NHS tend to:
-
- Mainly be interested in funding specific services rather than in ensuring that there is core funding to enable community anchors sustain their primary function which is being there to build meaningful long term relationships with people who statutory service often talks about as being ’hard to reach’.
- Focus on social prescribing – which places an emphasis on referrals coming from the health system first and often does not bring any funding.
What do you think?
The Bicycle Crash and Care Opinion

Here is my story
On the 28th of January this year I was cycling down Common Lane in Sheffield heading back home after having had a good time on a fell race nearby. My main objective was a pint of stout at my local. I had cycled this route many times – there is a very sharp right hand bend and I did what I normally do. I looked across the field to make sure that there was no traffic coming the other – so that I could pull out into the middle of the road in order to manage the bend.
That was the last thing I remember… until I came too … sitting against a stone wall by that right hand bend. There were four people gathered round me who turned out to be cub pack leaders from the nearby Girl Guides centre – they included a firefighter, nurse and policeman!
20 minutes later an ambulance arrived and took me to A&E where they checked my concussion, found my snapped collar bone (not difficult!) and cracked rib.
All in all it was a very positive experience from the NHS in Sheffield for which I was very grateful.
I did have a small concern about the sling I was offered at the end and the lack of instruction about using it.
A couple of weeks later I left a story about my experience on the Care Opinion website.
You can read my story on the Care Opinion website here
Shortly after posting I had responses from both the Yorkshire Ambulance Service and the Sheffield Teaching Hospital.
Both respondents asked me to get in touch. The Teaching Hospital wanted to follow up my positive comments and my point about the sling and the Ambulance Service wanted to know more details so that they could pass on my positive comments to the ambulance team.
What this means
I have commented before about Care Opinion here and here.
My personal experience affirms what I have thought about Care Opinion, Patient Experience and Service Quality.
The Care Opinion portal allows:
- The patient or member of the public to tell their personal story that reflects what happened rather than just ticking boxes or providing simplistic scores.
- Relevant services to establish contact with the patient and respond to feedback.
- Points of concern to be fed back to services.
- Praise for how services or people work to go back to relevant staff.
What I have learnt
The NHS is under tremendous pressure at the moment. A lot of the media has contributed to creating a hostile environment for people who work in the health system the vast majority of whom are doing their best to respond to peoples needs.
Patient Experience tools such as Care Opinion are an important way of communicating back to staff and services about what has gone well and what could be better.
In this hostile environment it is extremely important that NHS services use easy to use but powerful mechanisms such as Care Opinion to capture stories of patient and public – not least to ensure that there are robust channels of two way communication between the public and the NHS.
This helps empower staff to improve and to be assured that many of us value the work they do – this is so important now.
Finally.
My thanks to all NHS staff who helped me on the 28th of January …. and the cub pack leaders.
I have started wearing a cycle helmet!
WHAT DO YOU THINK?
Integrated Care Systems – Accountable? Transparent?

The irony of giving people hardly any time to respond to a consultation on transparency and accountability of Integrated Care systems seems to be lost on the Department of Health and Social Care (DHSC) Hewitt Review.
Their consultation was launched on the 13th of December 2022 and closed on the 9th of January 2023. I reckon that is 14 days working days to respond.
I have to say that I am confused because there was a DHSC enquiry in 2022 which covered very similar ground.
Here are extracts from two of the witnesses to that enquiry
Kings Fund

Local Government Association

Problems
Government seems to think that it is essential to restructure the NHS every 5 to 7 years. One of the consequences of this is that most people have little idea of who is making local decisions about what gets funded in the NHS and how to influence them.
Speaking as a former lay member of the Clinical Commissioning Group in Sheffield – There were still many people in Sheffield who had no idea what a CCG was by the time it was abolished. So the new ICS structures will be little understood by most people.
When Integrated Care Boards were established it was clear that their main accountability would be to themselves and to central government

This centralised control and constant reorganisation – can lead to a feeling that the only accountability that ICB leaders really need to worry about is to central government. This is so distant that control tends to end up focussing on activities that can be easily measured such as budget deficit, waiting times and ‘never events’.
It takes exceptional principled local NHS leaders to give equal weight to complex local challenges that cannot be so easily measured, inequality, lived experience, diverse needs etc.
I think it is really hard for public bodies – particularly the NHS – to admit that there are areas where they are struggling or have made mistakes. This is dangerous. In less than a year we have moved from praising primary care and the NHS to seeing the government and national media attacking them. This has contributed to antagonism from members of the public as they have struggled to access services.
In my view there is a shameful silence from local health systems – who have not pointed out loudly or clearly enough the demand, financial and quality challenges that are faced by front line staff.
This failure to do so creates a dissonance between what the local NHS is saying and what patients and staff feel they are experiencing.
In my recent blog on health inequalities and how Integrated Care Systems are using or misusing funds to tackle inequalities it was concerning that many readers complimented me on doing what is a comparatively simple piece of work – sending some Freedom of Information Requests and analysing the responses.
What was apparent was that many players in the local health and care system were:
- Not aware of the existence of these funds
- Did not know how to get access to this information
- May have known what was happening but felt unable to challenge or question decisions that had been taken.
This is worrying, not least because it is areas such as health inequalities and public voice that need informed scrutiny and public debate. If they don’t have this they risk continuing to being treated as marginal issues at best.
What can be done?
Here are some thoughts.
A high performing organisation must create mechanisms that challenge what it is doing both internally and externally. That is a key driver for improvement and excellence. Sweeping issues under the carpet will disillusion staff and reduce public trust.
Empower Staff
Organisations such as the Integrated Care Boards need to have internal structures that empower officers who are responsible for engagement, involvement and tackling inequality.
In Sheffield the Clinical Commissioning Group established a separate committee as part of its constitution where all decisions that required public consultation or involvement were sent. This committee considered the approach being taken by the commissioner – for example how were views being sought? Who should be involved? What actions needed to be taken to be inclusive etc. It was not about ‘marking the homework’ it was concerned with empowering the commissioner to make the best decision possible by ensuring that the views of key stakeholders were heard and understood. The Committee membership included public voice members (recruited through open open recruitment) Healthwatch, the local authority and as importantly Directors from the CCG, GP members and members of the involvement, equality and communications teams.
Empathetic learning
Integrated Care Systems need to establish inclusive action learning sets that create a safe and empathetic place for decision makers to honestly share the challenges that they are facing tackling difficult issues and be constructively challenged by peers.
Trusted relationships
There needs to be trusted relationships with different communities and stakeholders.
During the pandemic Sheffield CCG funded at least 20 voluntary organisations who worked with or came from specific communities – learning disabilities, BME communities etc to regularly share their concerns and challenges – with the ‘gold command’ in the city. There was a clear view from decision makers that this assertive relationship building helped Sheffield’s vaccine rollout be one of the best compared to other Core Cities. This approach is similar to the small grant programme run by Healthwatch in Sheffield.
Another great example is how Birley Health Centre have used simple mechanisms such as Facebook to create a platform for the honest sharing of criticism and praise. Most importantly it creates an ongoing relationship with patients at the practice, approximately 10% of patients are members of this group.
Building Capability in communities
Understanding and influencing complex short lived health systems is really hard! In Sheffield there is a long standing Introduction to Community Development and Health course – aimed at citizens from easily ignored Communities. In 2023 this course celebrates its 25th anniversary! Frankly any ICS that is serious about local accountability and transparency should be investing in these sort of local initiatives and taking advice from national organisations such as Citizens UK.
Scrutiny and Challenge
Local Authority health scrutiny committees have an important role here. However, I think that they can be significantly helped by partnerships with organisations who are independent and have the skills and expertise to analyse data quickly. A practical partnership with a university could help here – so long as they understand that they are using their skills to produce fast analysis that helps systems in real time!
Finally – of course there will always be a few old bureaucrats like me with a glass of wine and a computer who will write blogs sharing their opinions – but surely we can do better than that!
WHAT DO YOU THINK?

What do you do when you are allocated a tiny amount of funding to tackle a long standing and complex problem? There must be a temptation to spend it on other pressing challenges … on the basis that the funding would not make a great deal of difference anyway.
I think that this is one the dilemmas that integrated care systems faced when each received some funding specifically to address inequalities.
This spreadsheet shows the funding allocated to each integrated care system in England for 2022 – 2023, page two shows the specific funding allocated to address health inequalities.
The thinking behind this funding is set out in this document.
In Yorkshire the total funding to specifically tackle health inequalities was just over £22 million in 22/23. This sounds a lot – but equates to just under a quarter of one percent of total NHS spend.
Just to note I might have misinterpreted some figures – but I think my data is broadly correct – get in touch if you know better! More positively this is recurrent funding with quite broad criteria with regard to how it is used, this could provide an opportunity to develop strategic levers for system change.
More positively this is recurrent funding with quite broad criteria with regard to how it is used, this could provide an opportunity to develop strategic levers for system change.
So, lets have a look at how each of the three Integrated care systems decided to use their allocation. I have had responses to a Freedom of information request from each ICB in Yorkshire.
The full response for each ICB can be read below, I recommend reading the West Yorkshire one in particular because it is the most considered and comprehensive.
I have tried to summarise these responses in the table below

Summary for each ICB
West Yorkshire
Have well established structures, active involvement of a range of stakeholders including the local NHS, Local Government and the VCSE. Their actions are consistent with the Core20plus5 NHSE model. They have a decentralised model which balances local actions with sub regional activity when this is more appropriate.
Humber and North Yorkshire
Half of the funding has been used to underpin their financial plan. I interpret this as contributing to addressing the financial security (deficits) within the system. While I do not agree with using this funding in this way – I do welcome their honesty in declaring this. The approach they are taking with the remaining funding is consistent with some of the priorities within Core20plus5 but is quite narrow.
South Yorkshire
As the table above shows, South Yorkshire ICB approach feels vague. They are not able to identify their spending plans for this year – and now have less than 3 months to commit. It is hard to see how they will get the money out of the door. From the response it looks as though they are more focussed on next year. Unlike the other two ICBs it is hard to see what specific structures they have in place to drive this work forward.
Actions
Read this
Given the significant variation in actions across the three ICB in Yorkshire it is very likely that this inconsistency is reflected across England as a whole. This muddled approach is consistent with the findings of a piece of work by Olivera et al which flags up that work in local health care systems on inequalities is characterised by vagueness, lack of clarity and lack of commitment to action. This report is a must read for NHSEI and for integrated care boards.
More accountablity
It is very concerning that Integrated Care Boards are able to use this funding to address wider system funding problems by in effect raiding a tiny fund which is specifically allocated to develop actions to improve the health of the most disadvantaged. This is precisely the sort of behaviour that creates and deepens inequality. NHSEI need to establish clearer requirements to ensure that ICBs are held to account for decisions they take both locally and nationally.
Theory of Change
As the Olivera paper notes there is a real lack of clarity about what actions will have the greatest strategic impact and indeed what is meant by health inequalities. It does feel as though there is a lack of rigour here. There should be a clear requirement for Integrated Care Boards to each develop a 5 year theory of change which should underpin their health inequalities strategies.
What do you think?
Fading away? NHS Yorkshire action on financial insecurity

In my previous blog I looked at the response of the three Integrated Care Systems (ICS) in Yorkshire to the growing financial insecurity faced by many people in this region. Each Integrated Care Board (ICB) received a paper which set out the context, rationale and in the case of two ICS made a number of recommendations for action.
As I said in the blog – it is so important to come up with quick practical actions that will make a material impact on people who are most effected by a toxic combination of poor health, financial insecurity and a reliance on NHS services between now and the next two years at least.
It is important that ICBs recognise that local government and the VCS are under terrible financial pressure and their situation is likely to get worse. So just referring more people through social prescribing to welfare rights and debt advice is worse than passing the buck – it is irresponsible unless funding for these services is found.
I have now looked at the minutes of each ICS which captures the discussions in response to the papers. A summary of all the minutes is available here
The big danger is that after an initial flurry the financial insecurity crisis will be largely ignored as NHS systems default to focussing on the very real demand and quality issues in the health system – ignoring the feedback loop between health and poverty and forgetting their ambitions to take a ‘population health management’ approach in an ‘integrated care system’.
There is a tendency to default having ‘interesting’ discussions but failing to agree practical strategic actions. If any board is commissioning work try to understand the problem’ or is hunting for ‘evidence of what works’, it’s a sign that they have avoided taking action.
West Yorkshire minutes
Chair reminded the ICB that the Integrated Care Partnership (WYPB) asked for a response in relation to alleviating poverty.
Recognition that the ICB had two potential roles – for staff and for citizens in West Yorkshire.
Practical examples such as Winter warmth investment and link to tackling inequalities.
Call for development session for ICB
Recognition that work was going ahead in each place and it would be helpful to have oversight and assurance for this work
Actions
Board members invited to contact the Chair and Chief Executive to join a Task and Finish Group to take forward actions identified in recommendations.
Humber and North Yorkshire
Actions
A letter has been drafted by the Chair and Vice Chair (not in public domain) which will describe actions that are taking place and setting out best practice with regard to impact.
The ICB is looking to secure clear evidence in terms of impact and is working with local universities with regard to this.
It is expediting the approach to social prescribing and work with regard to workforce and recruitment.
South Yorkshire
Noted a fast change environment and worsening situation with regard to inflation. Concerns raised with regard to impact on cost of prescriptions, need for signposting to debt advice by NHS, impact on winter planning.
Concerns re NHS workforce impact with 40,000 earning less than £25k, focus on areas of deprivation not sufficient – eg people with learning disability, impact on local economy.
Concern that leadership on this is not clear – view expressed that ICB role is not about dictating or providing answers but contributing to solutions. Important to learn from COVID. Importance of working in collaboration with VCS.
Actions
Place directors to consider practical responses and report to October development meeting – I think this means a private meeting.
My conclusions
ICS responses to the growth of financial insecurity in their populations is unclear. There is a real risk that instead of meaningful strategic actions we will see a default to traditional pathways that appear to involve action but make little difference to population health.
The red RAG ratings to watch out for are – an over emphasis on:
- Role of NHS as Economic Anchor
- Focus on staff pay and conditions rather than wider population actions
- Focus on Social Prescribing to the exclusion of welfare rights services
- The awful OHID guidance aimed at making NHS staff more poverty aware
Actions we need to see
First, identifying populations who are using the NHS and at risk of financial insecurity and commissioning integrated welfare rights/debt advice to run alongside clinical services for example:
- Major Trauma
- Head Injuries
- Motor Neurone Disease
- Cancer
- Muscular Dystrophy
- Multiple Sclerosis
- People with acute mental illness
Second, commissioning of sessional welfare rights/debt advice services to run alongside GPs serving the most deprived populations in each place.
What do you think?

We are in for a very tough time over the next couple of years … and it will be the poorest who carry the greatest personal burden.
This is the time when the NHS needs to be looking hard at how it provides services so that they are delivered in a way that recognises the terrible financial pressures that people face.
I have had a look at the three Integrated Care Boards (ICB) in Yorkshire and was heartened to see that each had a paper which is specifically about the impact of financial insecurity on the health of the populations they serve.
Actions
Two of the papers – WYICP alleviating poverty report and Humber and North Yorkshire ICS had been discussed at the wider Integrated Care Partnership (ICP) too – this feels right, because the wider voluntary and community sector and local government already have a track record here.
The South Yorkshire paper has only been to the ICB so far – it’s more of a discussion paper – without specific recommended actions.
The other two papers suggest actions that include:
- We need to better at bringing population based data that is relevant to the ICS specifically on inequality and financial insecurity.
- NHS and care staff need to be provided with training and support about the impact of financial insecurity on their patients so that they can signpost and advise.
- Thought needs to be given to how access to welfare advice and support is given within key pathways.
- The role of the NHS providers as key economic anchors needs to be utilised
- NHS and Social Care staff who are experiencing financial insecurity need to be helped
Leadership
West Yorkshire and Humber and North Yorkshire recommend establishing strategic groups to keep a grip on this agenda and to be accountable for a response. Humber and North Yorkshire ICB has used their helicopter view to provide an appendix summarising approaches being taken in each place and by each NHS organisation. This is helpful although there is no overarching analysis of this.
What do I think?
The papers help, although they default too easily to rather grand system change ideas rather than focussing on actions that address the immediate crisis. For example talking about the role of the NHS as an economic anchor is fine but ain’t going to address current challenges. The reasons why the NHS needs to step up here is better explained by organisations outside the NHS such as Macmillan and the Money and Mental Health Policy Institute.
I think the NHS needs to focus primarily on practical actions that health systems can take now that will improve peoples financial insecurity and benefit the NHS. This will require cultural change and modernising what we think good clinical practice is.
Calls for more work on understanding population data better is probably a distraction. It is perfectly possible to establish a framework based on health impact/need for NHS services/financial vulnerability that can play to the strength of NHS clinical delivery models – by focussing on particular conditions and defined populations. The generally rather bland Kings Fund think piece has a good example of this below. I have written extensively on this using examples such as the Cancer, Major Trauma, Mental Health, Progressive Illnesses etc.
There is money
There is funding out there available to help people. The online advice service ‘entitledto’ produce a yearly analysis of how much benefits are unclaimed each year. Their estimate for 2022 is £15bn across the UK. This equates to roughly £1.2bn available for people in Yorkshire. I challenge any NHS ICS to propose an alternative course of action that would help people as significantly as enabling people to access these unclaimed benefits.
The reality is that vulnerable people experiencing traumatic health conditions need expert help to access the benefits they are entitled to.
I think that the NHS has a key role to play in helping get this money into peoples pockets by funding dedicated welfare rights services. There are too few examples of this – in Sheffield the NHS funds a welfare rights service specifically for people experiencing acute mental health problems.
Actions
We need an action plan which:
- is informed by services on the front line who are tackling financial insecurity and health. Such as national ones like Macmillan and the Money and Mental Health Policy Institute and local ones such as Local Citizens Advice.
- is about impact over the next 2 years
- invests NHS funding directly into welfare rights services that are integrated into key clinical services – not distractions such as social prescribing
- focuses on areas where the toxic combination of a significant health problem and financial insecurity impact on NHS utilisation and personal recovery.
- What do you think?
Disclosure – I am Chair of Citizens Advice Sheffield
Waiting for the South Yorkshire Integrated Care Partnership
UPDATE – 24th October 2022
Since I published this blog on the 3rd of October the original South Yorkshire and Bassetlaw ICS website has been updated. It now appears to be the platform for the new Integrated Care Partnership.
3 months after the NHS restructured we are still waiting for the South Yorkshire Integrated Care Partnership to be formally launched.
Quick Explainer
Since July 2022 Integrated Care Systems (ICS) are the way the NHS is organised. England has been divided into 42 sub regions each with an Integrated Care Board (ICB) – mainly focussed on the NHS and an Integrated Care Partnership (ICP) – with a broader strategic remit including local government and the voluntary sector.
ICPs are responsible for producing the Integrated Care Strategy for the ICS.
It’s the Integrated Care Partnerships that puts the ‘I’ in ‘ICS’
Integrated Care Partnerships are important, but there seems to be significant variation in the progress being made to establish this basic infrastructure that is part of Integrated Care Systems.
Lets have a look at Yorkshire (population 5.4 million)
In Yorkshire there are 3 ICS. Two appear to have an Integrated Care Partnership up and running with clear links to it via the Integrated Care Board these are West Yorkshire and Humber and North Yorkshire.
3 months into the creation of the new health structures the only mention that I can see of the South Yorkshire Integrated Care Partnership is an announcement that the South Yorkshire Mayor has been appointed Chair. There appears to have nothing up at the moment that the public can see – not even a note on the website saying that this is a work in progress, watch this space etc etc.
I think the resources and responsibility to establish the partnership rest with the Integrated Care Board not the Mayoral Combined Authority (MCA) … although it would be refreshing if the SYICB were to pass the resources for coordinating the Integrated Care Partnership over to the MCA.
Here are the screenshots from the three Integrated Care Boards showing how we can find out what the Integrated Care Partnership is doing, who is on it etc.
West Yorkshire

Humber and North Yorkshire

South Yorkshire

Meanwhile in South Yorkshire
I have heard informally it that the South Yorkshire Integrated Care Partnership had a private meeting in the week starting the 28th of September, and that Oliver Coppard the Mayor for South Yorkshire has been confirmed as Chair
However, at the moment it is not possible to know:
- Who is on this partnership
- What its agenda is
- What its forward plan for meetings are
Does any of this matter?
The government guidance is clear:
“The integrated care partnership MUST involve in the preparation of the integrated care strategy: local Healthwatch …. and people who live and work in the area.”
“In order to influence the first 5 year joint forward plans the integrated care partnership would have to published an initial strategy by December 2022”
In South Yorkshire we have less than two months for the public and communities to get there head around what an Integrated Care Partnership is let alone to then engage and comment on the strategy.
Current Position
This is how I rank the three Integrated Care Systems with regard to how they publicise the role of the Integrated Care Partnership
First – West Yorkshire
- a clear accessible website – that shouts their values.
- The website also makes it easy to click on the ICP pages – one click away!
- There are also clear links to the agendas and minutes of previous meetings. It is easy to find out who the partners are – with logos to each organisation that click through to the relevant website.
Second – Humber and North Yorkshire
- website nice & friendly
- it does take 2 clicks to get to the ICP pages
- the ICP link is a bit hidden in the Integrated Care Board Page.
Third – South Yorkshire
- nothing to see here!
I would be very interested to hear from people living in other ICS areas outside Yorkshire. How easy is information about your Integrated Care Partnership to find? Who is on it?
What do you think?
 As a resident of Sheffield I was keen to have a look at the newly launched “Start With People” strategy, which was approved at the first public meeting South Yorkshire Integrated Care Board (ICB). It sets out how the ICB will work with people and communities . Here are some thoughts.
As a resident of Sheffield I was keen to have a look at the newly launched “Start With People” strategy, which was approved at the first public meeting South Yorkshire Integrated Care Board (ICB). It sets out how the ICB will work with people and communities . Here are some thoughts.
The strategy is strong on principles – particularly with regard to the aspirations that the ICB has with regard to developing strong and trusted relationships with the public in South Yorkshire.
I was surprised but pleased to see a photograph of Dean in the strategy. Dean is the butcher I go to every Saturday down at the Moor Market. So when I popped down for some home cured bacon (which I strong recommend) and a couple of Barnsley Chops I showed Dean his photograph. Both Dean and his wife were surprised to see him in the strategy – they knew nothing about it and had not been approached for their permission. To be honest as I said to him, I was surprised too – I know that he has an excellent reputation for a finely cut piece of sirloin – but I was not aware that he had strong views on collaboration and co-design in the NHS.

There is a serious point here – if you say that your NHS strategy puts the relationship with the public at the heart of your work then you need to live by that. The photographs in this strategy are of real South Yorkshire people – yet it feels as though they have been used as stock images to bring a bit of local colour to give the report authenticity. That is not right.
Moving on….to inequalities
The strategy identifies a range of areas that the ICB will be focussing on here and references the NHSE Core20PLUS5 framework. However it is not possible to understand how the actions that are set out here relate to these. It is also hard to understand the relative ambition with regard to scale and impact here. These feel like a disparate collection of projects that have been hoovered up into this space.
What is lacking is an analysis that tells us what the problem is, its scale and the actions that the NHS will be taking to address it.
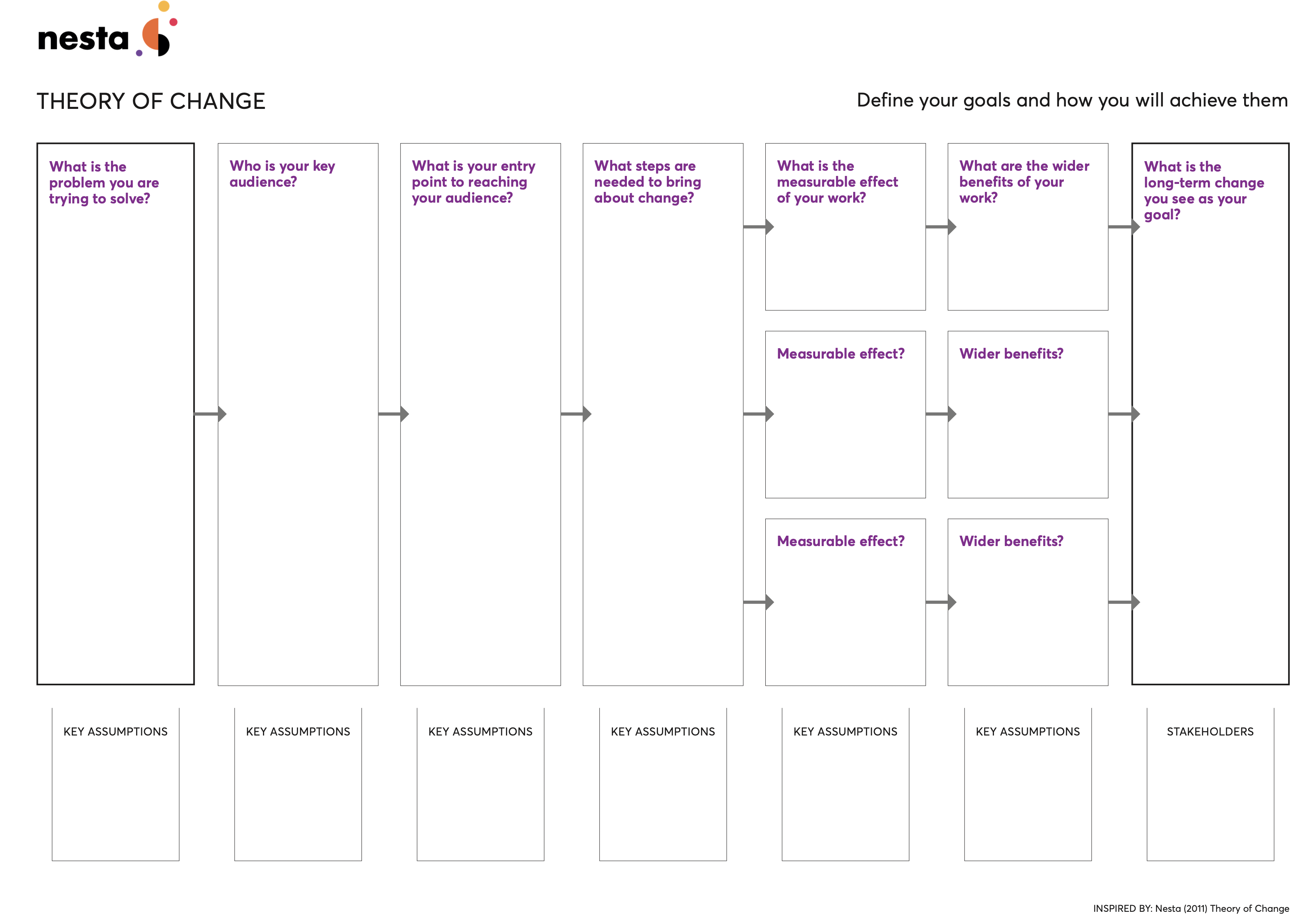
I think part of the reason for this deficit lies in the very simplistic “Theory of Change’ that the ICB is using – this is listed on page 38 of the report – and I show it below.

Most theories of change start by analysing the problem that needs solving – and then considering what the goal should be with regard to addressing this problem. Many – particularly when addressing complex whole systems problems also recognise that a key early step is to consider who needs to be involved, influenced or engaged in order to take effective action.
The (uncredited) theory of change in this strategy does none of these things. Sadly, I do think the NHS has history here – tending to default to project delivery planning tools when trying to achieve system change.
There are more appropriate theories of change – check out the United Nations one or closer to home – NESTA. Both have an upfront analysis of what the problem is – which for a new organisation with ambitions to be accountable and transparent would seem like an essential thing to do.
Finally! … a real problem
For me the most important paragraph in the whole document is tucked away at the end of the section on the Voluntary and Community Sector – page 9 – which states:

When I read this paragraph my thought were:
- Is this really the case?
- Why do communities distrust the NHS?
- Which communities distrust the NHS?
- What does this mean for the health of populations?
- What does this mean for the way that NHS are provided?
- What actions need to be taken to change this perception?
- And most importantly has the lack of trust maybe got something to do with inequalities?
So, coming full circle – yes, it is really important to be upfront about principles – but communities will not trust us if they feel that we are just playing lip service to how we represent and involve them and present unconvincing strategies to address the real problems they and the health systems faces.
WHAT DO YOU THINK?
