Talking about Community Anchor Organisations

At Leeds Beckett University we undertook a piece of work called Space to Connect which was funded by the department for Digital Culture Media and Sport and the CooP Foundation.
The programme was meant to look at how community anchor organisations could develop physical spaces to improve sustainability and services.
We had just started work when the Pandemic hit!
So instead we worked with these organisations looking at what they did during the pandemic to respond to the needs of isolated and vulnerable people in their communities. Many of us saw how community anchors pivoted and were among the first organisations to respond to need.
At the time there was a lot of hopeful talk about how this experience would represent a shift (some say a ‘left shift’) in how the local voluntary sector was perceived, funded and collaborated with by the NHS in particular. I think it is fair to say that there is still some way to go!
One of the products we produced was a discussion tool that can be used in a meeting or a workshop to begin an action focussed conversation within NHS organisations or an ICS about Community Anchor Organisations. The idea being that just having a conversation in a meeting would represent a useful step forward.
There is a blog on the Leeds Beckett website about this – which you can access here
If you would like to look at the discussion tool the link is here – ignore the first page – it is just the standard format used by Leeds Beckett when reports are stored on the website – it is much more attractive than that!
Finally, what was really important was our joint work with Locality which is the national organisation representing Community Anchors. The link to the Locality website is here
Do feel free to get in touch if you would like to know more.
Inequality and Left Behind Neighbourhoods

I recently spoke at the All Party Parliamentary Group Inquiry into Levelling Up which is focussing on ‘left behind neighbourhoods and feeds into the development of the Governments Levelling Up White Paper.
Here are a three things I learnt.
Unclear Actions
The best analysis I have seen is the one done by they Institute for Government, it’s nice and short and concludes ‘broad ambitions but … lacks focus’.
Money – this won’t touch the sides on the way down!
The Levelling Up white paper is full of commitments to funding and some of it sounds like quite big sums but its really hard to work out how real any of it is.
When I try to understand funding I ask the following:
- Is it new funding?
- Is it recurrent or one off?
- How much is it worth once it has been divided up into 151 unitary local authorities in England?
- How does the funding match up with what has been cut from local authorities in the last 10 years
- How does it compare to current local authority budgets
An example – the White Paper refers the creation of the £2.6bn UK Shared Prosperity Fund to be used to ‘restore local pride across the UK focusing on investment in improving communities and place, people and skills and supporting local business’.
£2.6bn sounds like a real statement of intent – this feels like big money! But when we look at the allocations we can see how small this fund actually is. Over the three years of the fund South Yorkshire will receive £46,132439.
If this fund were divided by population for the four local authority areas this equates to approximately £6.4m per year for Sheffield – for 3 years.
This still sounds like a tidy sum – but Sheffield Council is now spending £211m less every year due to government cuts over the last 10 years.
Despite the paper talking about the importance of local decision making even this small fund is not in the gift of local decision makers. 16% has already been allocated to the Department for Educations Multiply Programme which focusses on on local skill development for adults – specifically numeracy. The remainder then has to be allocated across three huge areas:
- Community and Place,
- Supporting Local Business
- People and Skills.
This funding is barely going to touch the sides on the way down!
Local Context and Decision making
One of the biggest challenges that the White Paper and the focus on ‘left behind neighbourhoods’ does not acknowledge is the local context. If we are going to create fairer places we need those with resources to behave more fairly and maybe even give up some of their funding to help hard pressed communities.
The problem is that those who are relatively better resourced are also under pressure! Look at the NHS – which is usually a bit better off than Local Government.
Dentistry – in some parts of the country it is increasingly difficult to access NHS dentists.
Here is what Healthwatch England and CQC say.
General Practice faces an increase in demand and a decline in recruitment and retention – here is what the BMA says.
Waiting Times for elective services have increased – here is what the BMA says.
What this means for inequalities and levelling up
We are in a position where about 30% of the population experience substantial health inequalities. If we are to take action at a local level this means reallocating resources within an area because the funding made available through the levelling up white paper is not sufficient.
If the whole of the local system is under pressure it will be extremely difficult to persuade key stakeholders within the local NHS such as GPs, Dentists and Hospitals to reallocate some of the general ‘whole population’ resources to focus on those experiencing the greatest degree of health inequality.
What can we do?
This might feel a bit wet – but I think it is really important that we ensure that local decision makers are honest and describe clearly how much resources are actually available for ‘levelling up’ this means using frameworks such as my 5 questions above – this particularly applies to the NHS commissioners and Integrated Care Systems.
What do you think?
The NHS Operational and Planning Guidance for 2022/3 sets out a significant target for the system level roll out of virtual wards.
Here is the target
“By December 2023 to have completed the comprehensive development of virtual wards towards a national ambition of 40-50 virtual beds per 100,000 population.”
According to my maths – England has a population of 56 million which equates to (560*45) the creation of a minimum of 25,200 virtual beds in England. According to the Kings Fund, England has experienced a significant decline in acute hospital beds and currently has just over 100,000.
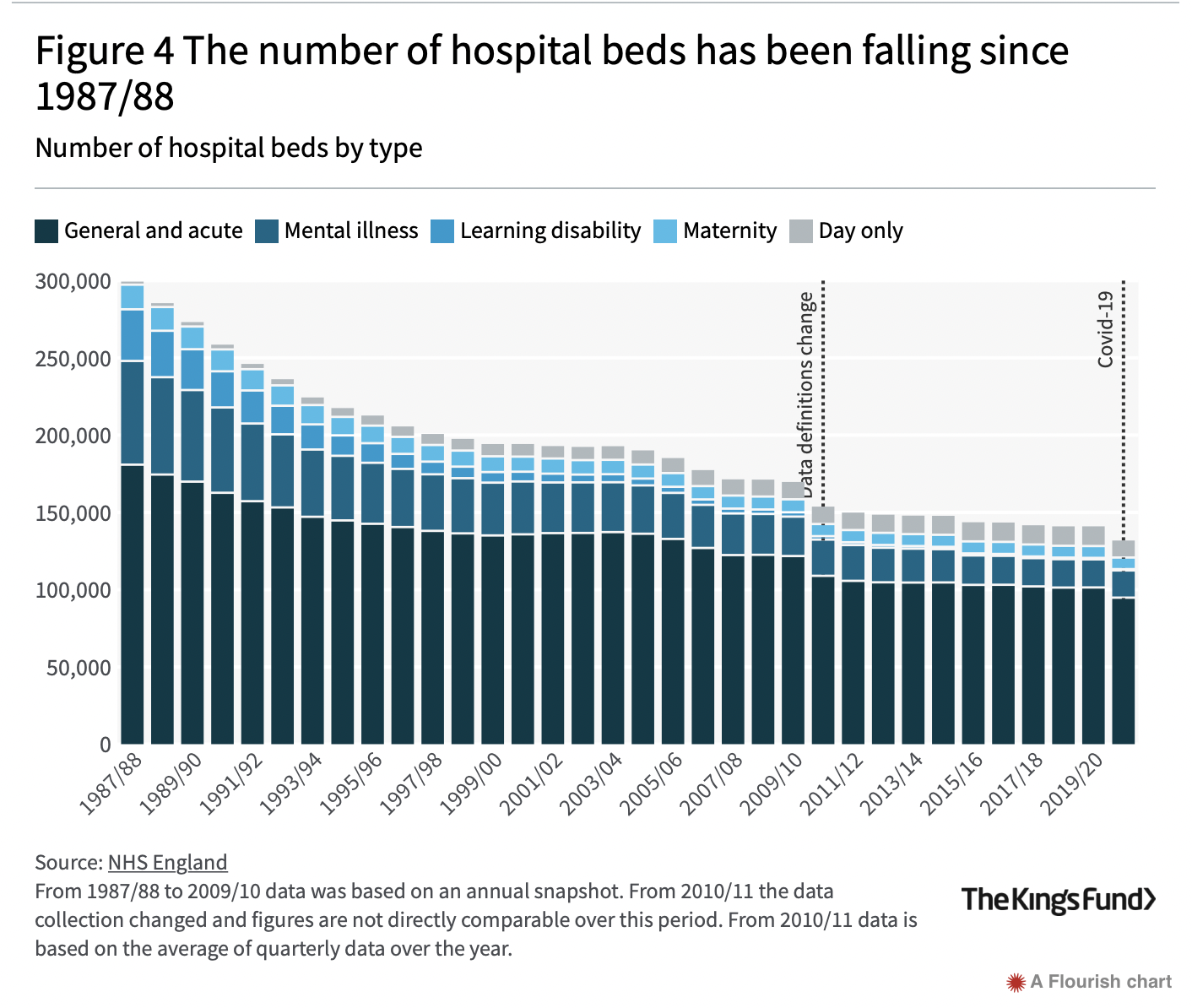
So this proposal equates to a 20% increase in beds – assuming that actual hospital beds are not reduced further.
Here is the money
NHSEI has allocated a total of £200m in 2022/3 and £250m in 2023/4 subject to targets being met (pp23/4 of operational planning guidance).
This £450m is transition funding only, and the second tranche of £250m has to be match funded by local systems in order to be released. This means that after 2023/4 local health systems will have to manage costs of running 20% plus beds from within their own resources.
The implementation costs equate to £450m/25200 = £17,900 per new virtual bed.
What is a virtual ward?
According to the NHS Supporting Information virtual wards:
“Support patients who would otherwise be in hospital to receive the acute care, remote monitoring they need in their own home or usual place of residence (I assume this means a care home).
..provide acute clinical care at home for a short duration (up to 14 days) as an alternative to care in hospital.
…are suitable for …. People with respiratory problems, COVID-19, heart failure or acute exacerbations of a frailty led condition”
What’s not to like?
I think there are two areas to be concerned about – which need more thought and action.
Inequality and Equality
The supporting information document I mention above is prefaced by a standard NHS statement – see below.
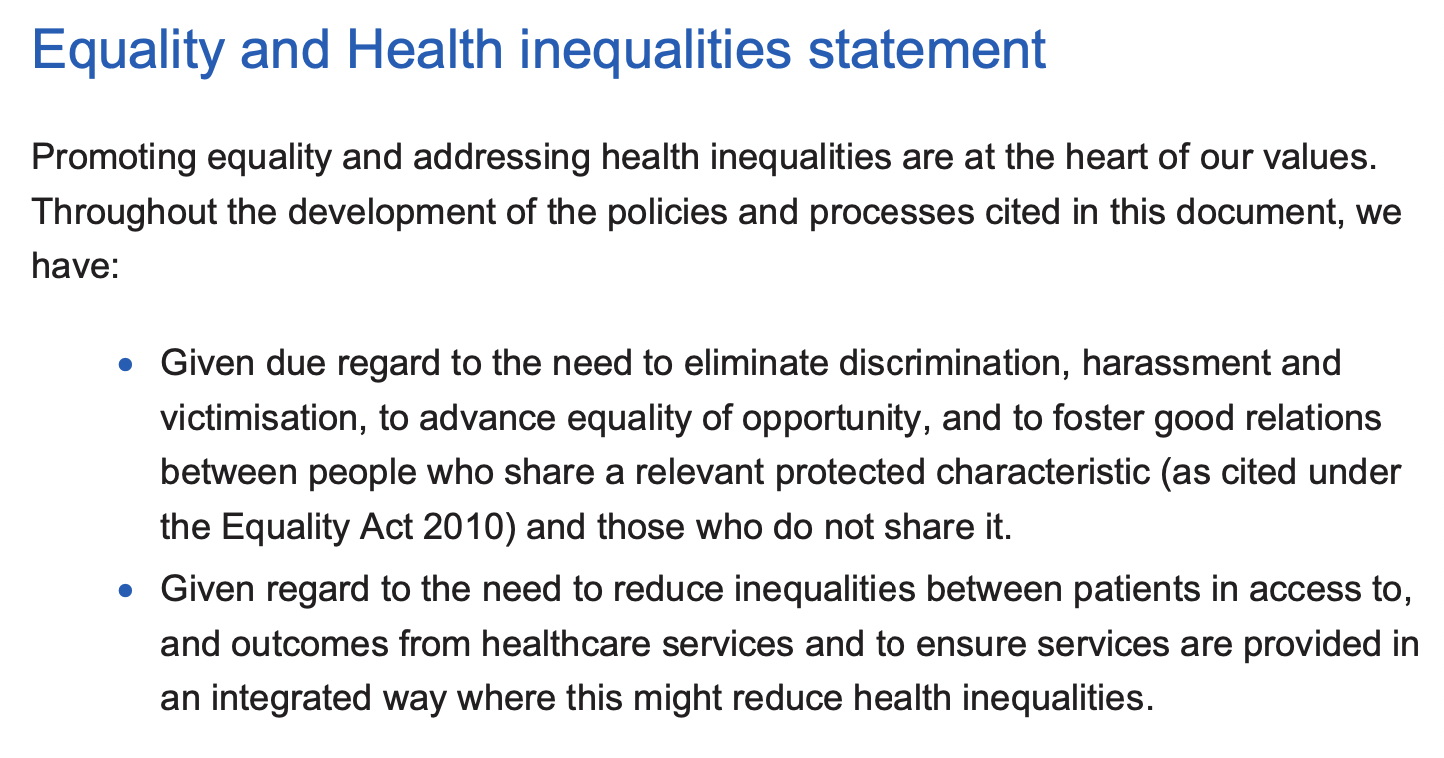
However the subsequent document makes no mention of why equality and inequality are relevant to this agenda and what actions might need to be taken with regard to the implementation of virtual wards.
Here are some suggestions:
The government has an ambition that 20% of acute beds will be provided at home in Communities. We know that:
- people with multi-morbidities are over represented in poorer areas
- Many people who experience health inequalities (core20plus5 group are more likely to live in poor quality housing, have low income and experience greater financial security
- The virtual ward model places a strong emphasis on digital connectivity -yet there is good evidence that disadvantaged communities lag behind with regard to access to digital technologies.
If we are to develop virtual wards in a way that does not widen inequality we need to consider how these will impact on people whose ‘virtual ward’ experience may be significantly worse than someone with a secure income, decent housing and good digital connectivity.
This leads me on to my second point…..
Integrated Health and Care systems
The current proposal feels like lifting and shifting a clinical model from a hospital to a community setting. Just because it is not in a hospital does not make it any more of a community based service – unless it is integrated into the local voluntary and community sector.
The ‘virtual ward’ patient is likely to require greater support from family or other carers, may require access to welfare rights and housing assessments etc. All of these can be addressed through a stronger funded connection with local voluntary organisations and local government etc.
What needs to happen
The NHS talks about the need to have a stronger focus on inequality and about shifting investment towards community and the voluntary sector, the virtual ward process needs to have:
- robust measures to understand the impact on inequalities
- have an explicit focus on capturing examples of good practice that address inequality and involve collaboration with the voluntary sector – this Leeds example looks interesting
- Costed plans to address the needs of patients living in poor conditions with fragile incomes
- Costed plans to ensure that the potential of the local formal and informal voluntary and community sector is utilised.
What do you think?
Talking and Learning about Patient Experience
In November last year I gave a lecture on Patient Experience to District Nurses, Health Visitors and School Nurses who are training at the Leeds Beckett School of Health.
I was lucky enough to be able to develop this in collaboration with the excellent Sarah Neill who heads up patient experience at Sheffield Clinical Commissioning Group.
Here are some of the things that I learnt and some information about a symposium we are planning for the 2nd of March this year.
We need to be clearer about what we mean by patient experience and why it is useful.
Finding out about how people feel about a service they received is generally seen to be a ‘good thing’. In the wider world of e-commerce leaving comments is increasingly understood as being useful. For businesses it can help them improve and promote their products, for customers it helps them avoid a bad service, find good ones and provides a way to ‘give something back’.
Yet, in the world of the NHS the use of patient experience feedback still feels to be inconsistent and its role poorly understood. I think this is for a number of reasons:
Top down
Many of the official or statutory methods for capturing patient experience feel as though they have little relevance to front line provision. In a number of cases this is because the perception is that these measures are really there to assure distant decision makers at the top of organisations or government that they know what is going on. Further, the relatively low number of respondents at a service or GP level can lead front line staff to feel that these are merely the views of an unrepresentative minority.
Resources
Health and care services are under unprecedented demand and have experienced real reductions in funding and a reduction in the rate of growth ever since the austerity imposed by the Coalition Government in 2008. For many clinicians there is a view that there is insufficient time and resource to develop patient experience while they are struggling to provide front line services.
Clinical training
I do think that some clinicians feel (after devoting years to professional training and ongoing CPD) that the reported experience of patients provides little added value to their practice.
The added value of patient experience
Despite the above challenges I think that systematically listening to the experience of patients is really important for the following reasons:
Validation and empowerment
Getting feedback on a specific action can be empowering. Most feedback to the NHS is positive. In the tough times we are experiencing with the pandemic, made worse by the actions of some of the press and government ministers it is so important that front line practitioners get to hear a different and often more positive view from people who actually use their services
Understanding the pressures that people face.
This quote is from a manager in an NHS Care Trust
“Can we look at the more social side of peoples lives – housing, isolation which may be the cause of or at least exacerbate a mental health problem. To understand experience properly do we need to understand it in the context of peoples lives?”
As we move to yet another reorganisation of the NHS one of the key words is integration – if we are to move to an integrated approach to service provision we need people to help us to understand how the social determinants of health impact on their health and there ability to use services.
The two quotes below come from a piece of work that Macmillan initiated to try to better understand what people with cancer were most concerned about.

Advocacy
Many NHS front line staff are working with defined populations of people (parents, a geographic community, people with a specific condition such as HIV or motor neurone disease etc). Understanding how this population collectively experience services and how these fit into the context of their lives can empower clinicians by providing them real stories of their patients. Clinicians can use these to advocate for service improvement and development in their organisations and with colleagues.
Join us!
As part of a wider piece of work Leeds Beckett are collaborating with the Patient Experience Library, with the support of NHS England and NHS Improvement to develop more training and support for people responsible for Engagement and Experience in the NHS and local Health and Care Systems. We are starting this work with a national symposium on the 2nd of March.
Why the NHS should be concerned about Poverty

The impact of inequality and poverty on health is increasingly recognised both within the NHS and among think tanks and policy makers.
It is important to catch this wave – this focus and interest is unlikely to last so we must make gains now to lay foundations for lasting change.
The new report by the Kings Fund on the NHS role in tackling poverty is an example of this. Over the last few years the Kings Fund has shown a growing interest in this area – although it still feels like a comparatively marginal activity in its work.
Their report is based on gathering together examples of existing practice in the NHS. This take us so far – but it misses some key elements that are essential for change to be long lasting. I wonder if the structure of the report has been constrained by contractual requirements from NHS England?
The biggest section that is missing in this report is asking and answering this simple question:
“Why should the NHS be concerned about poverty?“
If this is not addressed confidently and explicitly then we have not created a framework to have this debate within the NHS…… and a debate needs to happen.
The idea that clinical practice should be informed by the experience of poverty is still seen as irrelevant or at best a side issue by too many clinicians and directors of services
It is the Health Foundation who are doing the heavy lifting here.
The graphic below is from a Health Foundation article that sets out some of the reasons why the NHS should be interested in poverty. In essence it summarises some of the points made by Marmot in particular.

I think that there are three reasons why the NHS should be concerned about poverty
- if you are experiencing poverty you are more likely to be unwell and have multiple morbidities
- poverty means that you will find it harder to access services because they are too often allocated unfairly or are provided in a way that does not make it easy for you to use them because of where or how you live.
- a significant health problem creates financial insecurity and means that you need to use health services as effectively as you can – yet your poverty will make it hard to focus on getting well because you will be having to tackle financial problems such as debt or housing insecurity at the same time as trying to use NHS services effectively.
I summarise this in the poisonous Venn diagram below.

Over the years on this blog I have given examples of how a catastrophic health problem such as Cancer, Major trauma, Psychosis brings together this toxic mixture of financial insecurity, need for health services and difficulty in using them.
This combination is much more likely to make tough and resilient people vulnerable – it affects them AND it affects NHS services effectiveness. Here are two really good examples of work on this North East and Cumbria NHS – Poverty Proofing Health Settings and the Money and Mental Health Policy Institute.

I think we need to have a more systematic focus across health services generally, asking the question:
“where are some of the most vulnerable people in our hospitals and communities and do our clinical services reflect this need?”
Two final points.
It is dispiriting to see yet another report on poverty that devotes almost half of its suggested actions to the role of the NHS as an economic anchor. Yes, the NHS could do more on its role as a local economic engine – but putting it in this report is a mistake for two reasons.
First, the primary function of the NHS is its clinical responsibilities – giving this much space to the economic role takes attention away from this – imagine how barren this report would have been without this section? Frankly, we need that absence just to demonstrate how much further the NHS needs to travel here.
Second, we need a more considered analysis of the impact that economic anchors have on poverty. How much effect do they really have? Are there solid examples of where they have directly contributed to reducing or stemming poverty? It is too easy to get excited by the big money numbers without thinking … how much of this money actually ‘trickles down’ to those experiencing poverty.
Finally, we really do need to start talking more clearly about the role different parts of the NHS have with regard to the poverty agenda. We tend to default to just talking about community based services like General Practice and not give enough attention to the acute sector.
What do you think?
Reorganising the NHS (again) a failure of ambition, understanding and imagination?

Here we go again. NHS England are now in the final stages of reorganising the NHS along the lines that they flagged up in the 5 year forward view some 4 years ago. The report Integrating Care – Next steps to building strong and effective integrated care systems across England offers two options:
Either – make the current sub regional ICS partnerships statutory with a single CCG in each sub region
OR
Get rid of CCGs entirely and make the Integrated Care System a statutory organisation responsible for managing the allocation of funding at place (local authority level)
The second option is the one NHSEI want.
As usual the solution the NHS takes to wider societal and policy problems is to ……reorganise.
I am not going to spend the rest of of this blog complaining about the decision. I want to focus on the deficit at the centre of these proposals. During the pandemic one of the most important lessons that emerged is the primacy of place. This report recognises this – it talks a lot about ‘subsidiarity’, primacy of ‘place’ and ‘neighbourhood’.
However, the report does not appear to understand why this is important. It is locked into a simplistic and old fashioned view that the NHS is a bundle of services that are packaged up to be delivered at local authority, neighbourhood and subregion – it assumes that the challenge is one of technical delivery – rather than a negotiated relationship with all local stakeholders including the public.
No understanding is shown as to why local accountability, scrutiny or co-production is essential.
The reality is and should be that places have to make the tough decisions which requires local accountability. For example, in Sheffield there was an extensive consultation by the CCG on reorganisation of the Urgent Care system – which mobilised many groups in the city – mainly in opposition. This included regular lobbying of the CCG Governing Body. This pressure lasted for months – and was a constant reminder and challenge to the CCG that its analysis of the problem, the actions it was proposing and the way it communicated them was not good enough. At the end of this process this accountability and engagement ensured that the CCG listened and took a more thoughtful approach with regard to this agenda.
I am not convinced that the NHSE model – creating provider partnerships at place level provides the relationships, the longevity or the accountability that a corporate body with a board discussing difficult issues in public does.
Partnerships are not an effective mechanism for public accountability.
We only have to look at the current ICS model (where accountability rests with each member) to see how hard it is for the public to engage and influence Integrated Care Systems and Sustainability and Transformation Partnerships, yet this seems to be the model proposed for partnerships at place level.
What can we do?
- First, in order to make better decisions local NHS provider organisations must create a budget to fund a local independent function that will test and challenge local health and care decisions. This will be crucial – not least by providing resources to citizens who will want to engage with local decisions and with those of their ICS. This independent function could sit in local Healthwatch, Local Government scrutiny services or even with an academic institution.
- Second, provider organisations at a local level need to invest in a collective approach to building citizen voice to ensure that the way in which patient and public experience of health services is heard is significantly strengthened. This must include investing in VCS organisations who work with communities of geography and interest particularly those who are easily ignored.
- Third, we need an honest assessment of how Primary Care Networks are going to connect with communities. Mechanisms such as Patient Participation Groups have had very little impact – if PCNs are to be the point of connection with communities we need to be clear about how much of this local relationship building can actually be done by Primary Care Networks.
- Fourth we need to build robust strategic structures embedded in local authorities where membership includes councillors, supported by senior officers, NHS leaders and public voice membership (lay members). These need to control significant proportions of NHS and local government spend – for example in Sheffield the Joint Commissioning Committee is in charge of the £.5bn Better Care Fund allocation.
We will need to build these mechanisms not only to make better decisions locally but also to ensure that a stronger place based voice is heard in public at ICS level.
What do you think?
Levelling up our Communities – the paper Boris Johnson commissioned

Anybody interested in communities, citizens and their relationship with local systems must read Danny Kruger’s report “Levelling Up Our Communities” which came out in September. Danny is the conservative MP for Devizes – and has a track record of working in this area. I got to know him a bit because he was one of the people involved in the development of “A better way” a couple of years ago.
His experience and the fact that he appears to have the ear of the Prime Minister means that this report is worth a read.
The report like the Teresa May Government’s Civil Society Strategy (Danny was one of the architects of this) is a mixed bag and like that strategy contains too many little actions, lacks a clear theory of change with little clarity about the end point, priority actions and timescale.
Danny is honest about some of some of the policy challenges and failures:
- He recognises the scale of inequalities and the disproportionate effect that this has on communities and that ‘social safety nets that help people in crisis are fraying’.
- He acknowledges the lack of traction of Cameron’s Big Society initiative
- He notes the relative lack of success of the NHS Volunteering scheme to connect willing volunteers to meaningful activity.
If you would like to see positive if equivocal responses to this report there is a good summary here. While the report is full of ideas, I will focus on three areas that worry me – Local Government, Sound bites for the PM and investment.
The lack of focus on local government fatally weakens this report
The most important enabler – Local Government is barely mentioned, yet the report recognises that some local authorities have led the way with place based approaches that foster community volunteering.
I strongly recommend reading the latest excellent paper from New Local (Think Big Act Small) which does a good job recognising the crucial role of local government.
In fairness I suspect that Kruger has not focused on local government because of plans for a White Paper on the future of Local Government. Nonetheless, this absence sits uneasily with his suggestion of a Community Power Act which aims to ‘affirm the right of ordinary people to affect change in their neighbourhoods.
Recommendations the Prime Minister would like
There are some actions that I think will land well with a prime minister who likes big ideas and populist statements. Some of these include:
- A ‘Neighbour Day’ bank holiday
- Establishment of a ‘National Volunteer Reserve’
- Creation of a ‘Volunteer Passport’
- A Kickstart programme to pay young volunteers
All of these make nice headlines but I am not convinced that they are of strategic importance.
Where is the money?
The paper acknowledges the financial stress that the local voluntary and community sector have experienced. However the report feels constrained by an ideological view that the state should not be a long term or substantial funder of the voluntary and community sector. There is a contradiction here – given that the government has no ideological problem pumping large amounts of tax payers money into the private sector often with little scrutiny (See here, here, here). Further – local government (see earlier point) has a long tradition of funding the local voluntary and community sector through contracts and grant aid.
So, the report offers a patchwork of proposals which primarily see the government as an enabler not a funder – they include:
- Selling off public sector assets – is this seriously a long term plan?
- Persuading the wealthy to give more – good luck with that!
- Using the National Fund to create a Community Recovery Fund – currentl value about £.5billion. However, this is still only half the size of the Health Foundation – which while big is very small in terms of the scale of the challenges faced.
- Using dormant insurance accounts – value £2bn – is this really a long term funding source?
- Encouraging the faith sector to raise more money through fundraising – with a promise that this will lead to closer collaboration with government. I did a double take with this one. First, I thought that Government’s role is to work with citizens anyway (although the faith based Trussell Trust may disagree); second, is the paper seriously proposing that if an interest group raises lots of money they will get more influence on government policy?

What Next
Credit to Danny Kruger for setting out his ideas – he does want to strengthen citizen activism and assets – and he sets out an approach informed by his own experience, values and analysis of what is possible.
I think that those of us who are concerned about this need to respond to the opportunity created by this report; build on his analysis but also offer up alternatives to some of his proposals – there is a better way!
What do you think?

While we have our heads down in the pandemic NHS England is pressing ahead with its plans to reorganise the local NHS landscape. It looks like this involves getting rid of place based Clinical Commissioning Groups and creating sub-regional Integrated Care Systems and locality based Primary Care Networks. Much of this is in line with a blog I wrote 16 months ago.
NHSE has been held back because abolition of CCGs requires a change in legislation – which has been delayed by Brexit and COVID.
Nonetheless NHSE and the Government still appear to be keen to progress this – so instead they are using changes that do not require legislation retaining CCGs but reducing their number through mergers, with the aim of eventually creating a single CCG function that is co-terminus with Integrated Care Systems.
The current state of play is set out in this presentation which includes two examples from Norfolk and Kent showing how CCGs have CCGs have managed the politics of this change with local government and the public.
Although NHS England and the Department of Health and Social Care have said that choosing to merge is a voluntary process and will by decided by local CCGs it is of course possible to ‘encourage’ this by changing the wider environment through a mixture of incentives and pressures – for example:
- Require CCGs to reduce management costs by 20% by 20/21
- Claim that CCGS are volunteering to merge into sub regional ICS – in fact many mergers were due to CCGs wanting to become co-terminus with local authorities eg Leeds from 5 to 1 and Bradford from 3 to 1 etc
- Trying to create single Accountable Officer positions in charge of multiple CCGs on an ICS footprint – which is in effect a precursor to merger.
All of the changes above – taken by themselves can be seen as reasonable and only of internal concern to the NHS, which means that there has been little discussion of the direction of travel outside the NHS with local authorities, the VCS etc. The risk is that a series of much more important questions are left unasked and unanswered such as:
- What are the challenges facing local health and care systems?
- What are the best ways to mobilise a range of diverse stakeholders (the public, NHS, local government the private sector and the Voluntary Sector) to work together to address these challenges?
- What is best done at a neighbourhood, place, sub-regional and national level?
- What is the best way to hold these different stakeholders to account in order to bring supportive but critical challenge?
Why is any of this important?
There seems to be two assumptions within the NHS England/Government plans
That running the health service is best done at a sub-regional level with an implied belief that delivery of the health services is fundamentally about the management of standardised services rather than co-design of health and wellbeing systems to fit places. There also seems to be a belief that accountability to NHS England or Government is more important than accountability to places.
One of the examples in the presentation claims a range of benefits such as being better at tackling inequalities to justify mergers. This is a dog whistle argument – mention the right areas – but don’t present the evidence for why this is the case. This direction of travel – moving to get rid of place based CCGs to sub regional ones shows a failure to understand the contribution that local governance makes to collaboration and the development of integrated working.
In my experience the involvement of CCG Governing body members (Executive, GPs and Lay members) are key to connecting with the VCS, Health and Wellbeing Boards, Healthwatch, Joint Commissioning Committees and local authorities. This diversity of stakeholders has helped to build relationships, sensitise plans and strategies on difficult areas such as inequality, public voice and provided leadership in public meetings connecting citizens and communities to plans.
Second building on the CCG role at place level means that there is a good fit with local authority structures and accountabilities – this is how we do local democracy. It’s not perfect – but it is certainly better than moving everything up to sub-regions. As the paragraph below from the report of the Governments Public Accounts Committee in 2019 in 2019 on CCGs notes:
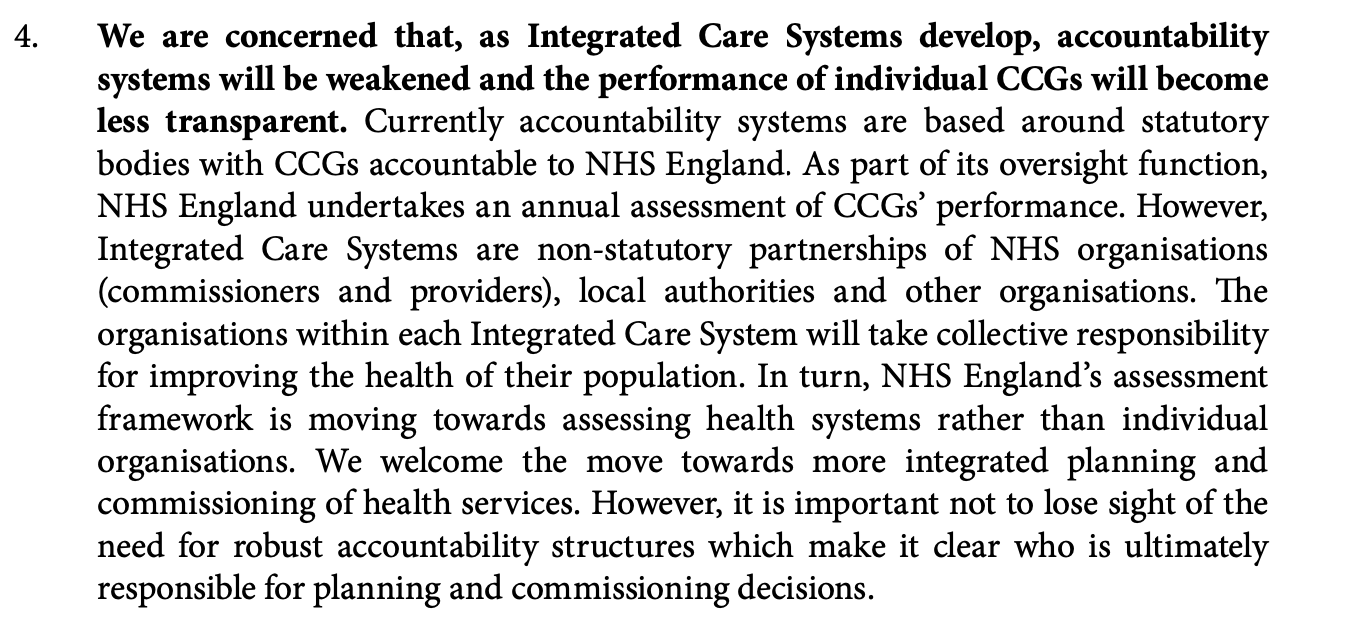
A similar and wider range of concerns has also been expressed by the British Medical Association in their 2019 guidance here.
What next?
Place based CCG Governing Bodies have either spent the last 7 years or so messing about or have (sometimes painfully) provided an important contribution to the development of local health systems – I think it is the latter! We need to:
- Set out with our local partners why place based governance of the NHS is important.
- Engage with their Integrated Care Systems – and ask the sort of system questions that I sketch out in bullets above.
- Where it does not already happen CCGs, Healthwatch and Local Government should be demanding that Integrated Care Systems have active representation from Local Government and the Voluntary and Community Sector – a good example of this is West Yorkshire and Harrogate Integrated Care System
What do you think?
Declaration of interest – I am a lay member on Sheffield CCG
I recently interviewed the board members of an integrated care system. This piece of work has challenged my ideas about how we best address health inequalities.
When it comes to tackling health inequalities I have tended to focus on those people and sectors who are most passionate and engaged with this agenda. Namely, the voluntary sector, general practice, communities themselves and local government. I continue to think this is important. However I think that we have ended up leaving the most powerful part of the local health and care system out of the discussion – the acute hospitals.
This has been a mistake.
Our expectations of what the acute acute sector can do with regard to health inequalities has been too narrow. When the acute hospital sector does engage it tends to default to rather limited outward facing areas:
- Local purchasing plans – citing the Social Value Act as an important lever (relying on the social value act is, in my view the last hope of the desperate!)
- Local transport to and from the hospital – again this is a usually more aspiration than action
- Local employment strategies – there are some promising examples here – for example the Leeds Teaching Hospital had a very successful local recruitment campaign in a deprived part of their patch.
All of these actions leave the most important part of hospital provision – clinical services – off the table!
It is comparatively rare to find examples where the hospital has taken responsibility for designing and leading a service that aims to improve a patients health in the round – generally hospital services focus on delivering a specific clinical intervention that ignores the context within which people live.
When a hospital does take a more person centred approach – magically – services becomes sensitive to health inequalities! Here are three examples:
London Homeless Pathway – Pathway helps the NHS to create hospital teams to support homeless patients and in some hospitals, Pathway Care Navigators: people who were once homeless to support homeless patients.
Major Trauma Unit Sheffield Teaching Hospital – A dedicated welfare rights service provided by Citizens Advice Sheffield for patients at the major trauma unit – funded by the Sheffield Hospitals Charity.
Guys and St Thomas’ Hospital Charity – take a place-based approach, addressing a small number of complex health challenges at a time. They work with local partners in Lambeth and Southwark and share their findings with others tackling similar issues.
We need to develop a new narrative that recognises the crucial role that acute hospitals should play here. Rather than trying to develop strategies that seek to ‘pull’ funding out of the acute sector we need to recognise the role of the acute sector and expect and support them to change.
What these examples tell us is that it is possible to work with clinicians to create a more inclusive model for good clinical practice, by recognising that the wider context of peoples lives affects their ability to engage with clinical services which then impacts on their health and how quickly they get better.
Here are some suggestions:
- We need to engage with Acute Hospitals and work with them to develop their own Health Inequality Action Plans that link their services to the wider population and the circumstances they face.
- The work of Guys and St Thomas charity provides insights into what this might mean but we need to go further. For example services such as Accident and Emergency should be used as a bellwether for local health systems – who uses them and why are indicators of socio-economic pressure and wider health system failure – I don’t think that local health systems use this data systematically or effectively to help shape wider strategies.
- The examples I gave above with regard to homelessness and major trauma show that a more inclusive version of what constitutes good clinical practice is possible. Both of these examples affirm that good clinical services must recognise that a patients vulnerability and lack of personal agency can be affected by factors outside the hospital environment. These examples show that good clinical practice inside hospitals involves more inclusive actions which can improve a patients ability to use health services effectively, help their recovery and be more cost effective.
Finally, there is of course added urgency here – the over representation of people from BAME and deprived communities among those admitted to hospitals during the pandemic and who now face long periods of recovery; must provide a further spur to considering how to develop inclusive services that respond to the clinical and social needs of people who have experienced a traumatic illness.
What do you think?
Two weeks ago Citizens Advice Sheffield shifted to only provide advice and support by phone and website to the people of Sheffield during this pandemic. All of this data comes from a report compiled by Citizens Advice Sheffield Chief Executive Clare Lodder.
Employment – Employment is now our 4th highest enquiry area (after benefits, universal credit and Debt) with enquiries for final quarter of the year running at 61% above the same period in the previous year.
There has been a steep rise in people seeking help with issues to do with their employment including problems with their employer in relation to what money they have received or how the job retention scheme is applying to them or short time working. (This has included a few employers who are confused about the scheme and unsure where to get information on this).
Sick Pay – We have also seen a spike in enquiries from the self-employed and enquiries about Statutory Sick Pay (both whether it should be paid and complaints about it not being paid).
Benefits – Problems with benefits including claiming universal credit – our Help to Claim team have a clear focus here and are able to give targeted help – but we are also helping with clients worrying about personal independence payments, particularly renewals and concerns over benefit payments.
Debts – Concern over debts, including council tax and fuel debts and an upsurge in enquiries around debt deductions from benefits and people with overpayments of Universal Credit
Destitution – People in need of help because they have no money to pay for food and/or fuel, usually because of benefit delays and the 5 week wait.
Local Collaboration
Citizens Advice Sheffield is working closely with all of the emerging support across the city including Sheffield City Council’s COVID response phone line and the local support and community hubs. It does feel that the city is now moving to a phase where there is much greater integration between voluntary sector and local government provision.
Our biggest concern
The biggest concern we have is to do with the inequalities aspect of this pandemic. Evidence from New York shows how unequal the impact of corona virus is.
People who were already on the the minimum wage – who are now finding that they have to manage on even less because they no longer have a job; people who are continuing to work because they need the income – in many cases they are providing ‘essential services’ such as public transport (this data on coronavirus deaths for public transport workers is appalling), supermarket retail, residential care, refuse collection etc.
Broadly the advice trends we are seeing are in line with the emerging picture from Citizens Advice nationally. Across the whole service in England and Wales, we are told
- The number of cases referencing coronavirus have doubled in local Citizens Advice service, and continue to increase in the consumer service
- Universal Credit remains the top issue for clients accessing local Citizens Advice, closely followed by employment advice
- The national website has just seen its busiest week ever with 2.4 million page views, surpassing the previous weekly high of 2.2 million page views.
Citizens Advice nationally has focused on rapidly updating its information on the public site.
What needs to change
Whilst Citizens Advice Sheffield have welcomed the Government’s announcements in relation to the help being provided, from the evidence from people we are helping, we believe there is more that should be done and in particular:
- Removing the 5 week wait for universal credit to be in payment
- Suspending all other benefit renewal action
- Extending the limitation date from three months to six months for enforcement action against employers who have failed to pay final pay
- Ensuring that there is a local safety net (for example by extending the scope of the local assistance scheme) to give money to people who are destitute because of benefit delays or other problems with benefits.
We also hope that some of the changes to the benefits system which have been introduced as a response to this current emergency are embedded for the future.
What do you think?

{kind=link}