
In our work with local Healthwatch it struck me is that one of the challenges that local Healthwatch face is operating at both an operational and strategic level.
The default for understandable reasons tends to be towards the operational – not least because I suspect this is what they are performance managed on by their commissioner. In other words there is a focus on the delivery of services. In Healthwatch terms this might be:
- Providing information and advice
- Undertaking a set of investigations in areas where there is concern – for example on provision of urgent care or dentistry or a programme of enter and view.
All of this is clearly important – a local Healthwatch has no credibility if it cannot demonstrate that it has a clear programme of practical actions developed in response to concerns raised by members of the public.
However, this is not enough – they need to be able to bring their influence to bear at a system level too.
In the Quality Statements that we developed for Healthwatch England last year local Healthwatch identified that one of the most important areas by which their effectiveness should be measured was that concerned with how they manage strategic relationships – their relationship to their local health and care system as a whole.
In order to do this effectively local Healthwatch need to go further than just using their positional power on the Health and Wellbeing Board. From our work I have seen examples of where local Healthwatch are doing this successfully. Here are some examples.
Making Quality Accounts Meaningful
Following a report we wrote on with Healthwatch Leeds on the relationship between Quality Accounts (and Local Accounts) and local Healthwatch – Healthwatch Leeds have continued to develop work in this area. This year they are holding two workshops – the first held earlier this year gave Quality Account leads from across the system (big hospital trusts, hospices, community NHS trusts, the local authority) the chance to share progress they had made to address some of the challenges they identified in the Quality Accounts last year. The second workshop will allow a joint discussion on their draft Quality Accounts for this year.
This friendly, collective discussion achieves the following:
- Sharing of good practice – its interesting that some of the work that the two Hospices were doing was of particular interest to the much larger NHS trusts.
- Breaking down silos – this is one of the few places in the local system that brings organisations together to look at how they connect and work together to meet the health and care needs of people in Leeds.
A shared approach to engagement
Healthwatch Leeds pulls together a “Public Voices Group” a regular bi-monthly meeting of engagement leads from across the health and care system – provider and commissioner. This forum provides an opportunity to:
- Share information on emerging consultations
- Discuss good practice
- Jointly publicise activity
- Undertake joint work – the group recently asked us to undertake a quick survey which looked at how different health and care organisations in the city used membership databases to connect with the public.
Advice and Information
This is an emerging area. In our work across the country it has been striking that the area where the work of local Healthwatch is least understood is that to do with Information, Advice and Signposting for individual members of the public. I don’t think this is surprising for two reasons:
- First, local Healthwatch are very small – in most cases there contribution to information and advice provision when compared to a large hospital trust, a local authority or welfare rights service is very small. This does not mean that it is not important. A local Healthwatch may be the last port of call for people who have struggled to get advice and information anywhere else.
- Second, in most local authorities areas no one has a handle of the level of advice and information provision in the health and care world and I have seen no evidence that anyone has an analysis of what good might look like.
I think that this could be an area where local Healthwatch has a role to advocate for a strategic review advice and information provision – who is being missed out and what good might look like.
What do you think?
Getting value from local voluntary organisations

You can’t buy long term relationships with short term contracts
The growing recognition of the importance of relationships, user experience and public voice highlights the urgent need for commissioners to look more closely at their culture and behaviour.
Although there are exceptions it too often feels as though the main mechanism for ensuring value with small voluntary sector organisations is through using 3 year contracts (sometimes with a roll over year) at the end of which commissioners go back to the market and tender again. I think this is often destructive and fails to capitalise on the opportunities presented by ‘local’.
Its not as if there were no other examples:
- Its quite usual for an NHS hospital to have at last a 5 year contract to deliver a particular service agreed with a Clinical Commissioning Group
- Most GPs have no fixed contract period
- Academies are offered 125 year leases on local authority schools and land for a token amount
- Commissioning organisations like Clinical Commissioning Groups work have no specific length to their existence or roles
All of the above are subject to a range of measures, performance systems, inspections, challenges etc that are used to ensure quality and value for money – the main mechanism is not market testing.
Short contract periods are often used because they are believed to be cost effective methods that can be used to assure the public that value has been achieved.
This is quite different from actually achieving value!
I worry that:
- A reliance on market testing and 3 year contracts takes responsibility away from commissioners of services to engage and foster collaboration with providers to ensure value.
- Is often used unthinkingly for local relational services – like Healthwatch – which rely on time to build relationships with members of the public and local organisations
- It does not take account of the strategic role of key smaller services such as Healthwatch confusing size of investment with strategic relevance and therefore allow system leaders to pass responsibility for quality assurance to comparatively junior contract managers who lack the position and strategic position to adequately assess competence.
The balance is of course shifting once again with a greater emphasis on localism and on new structures such as Accountable Care Organisations that seek to build relationships across different providers and with communities. Nonetheless, there is a risk that the emphasis here will be on relationships between the big players – leaving smaller voluntary organisations at the mercy of cruder mechanisms like fixed term contracts and tendering to ensure value.
Solutions?
Evidence and Collaboration
The work we have been doing with Healthwatch England starts to go some of the way to trying to address – using a 360º stakeholder survey that the contract manager/commissioning lead can use (in partnership with local healthwatch) to capture the views of wider players at both an operational and strategic level and then get a system level discussion going that generates a shared view of actions that can be taken to increase effectiveness not just by the local local Healthwatch but by all health and care organisations in the local system.
This sort of model can be used to gather a more sophisticated view of similar small VCS organisations whose role is complex, multi-sectoral and relational. For example community anchor organisations whose contribution is often ‘chunked up’ and defined by separate contracts that fail to capture the relationships, processes and added value. Its important to note that the Scottish Government is moving ahead on making core grant aid infrastructure funding available directly to Community Anchors.
Contract and Grant Aid – theory and models
There remains a crying need for local government and Clinical Commissioning Groups in particular to develop a more sophisticated view to how to best to ensure performance and value. There needs to be an urgent review of funding and performance levers that considers the respective roles of:
- Small and larger grants
- When fixed term contracts work and what length they should be
- What skills and capabilities local systems need to have in place to drive transformation and value
What do you think?

When a system is under pressure a natural tendency is to focus inward at precisely the time it needs to be looking outwards. So its not surprising that this report focusses almost exclusively on the NHS.
The Independent Mental Health Taskforce to the NHS in England report is a determined attempt to raise the profile of mental health services and in particular contribute to action that drives parity of esteem for mental health.
The foreword says:
“we have placed a particular focus on tackling inequalities. Mental health problems disproportionately affect people living in poverty, those who are unemployed and who already face discrimination. For too many, especially black, Asian and minority ethnic people, their first experience of mental health care comes when they are detained under the Mental Health Act, often with police involvement, followed by a long stay in hospital. To truly address this, we have to tackle inequalities at local and national level. ”
The problem is when I look through the report I cannot find this ‘particular focus’.
Inequality
The report does say that inequality is a major cause of poor mental health:
- People with mental health problems are overrepresented in high turnover, low pay and often part time or temporary work.
- Children from low income families are are 3 times more likely to be at risk.
- Children living in poor housing have increased chances of experiencing stress, anxiety and depression
- People in marginalised groups are at greater risk – especially people from black and minority ethnic communities
- As many as nine out of ten people in prison have a mental health, drug or alcohol problem
System Failure
The report does make the case for system failure:
- Three quarters of people with mental health problems receive no support at all
- There is wide variation in access to services such as IAPT – with waits of 6 to 124 days
- 20% of people on the Care Programme Approach have not had a formal review in the previous 12 months
- Mental Health accounts for 23% of all NHS activity but spending on secondary mental health services is equivalent to just half of this.
An argument for funding for NHS providers
The recommendations largely miss out on the root causes of inequality and primary prevention and instead focus on the system at the end of the line – the NHS – social care is poorly represented in the report.
There are almost 60 recommendations. With the majority concerned with local operational matters – how services are delivered, yet the report speaks primarily to NHSE rather than local health and care systems.
I am not saying that this huge wodge of recommendations are bad – but I think the commission ended up not seeing the wood for the trees – it has produced a plan that is about operational change rather than system transformation.
Missing the point
Inequality – The report is unclear about inequality – there is no challenge to how government policy risks exacerbating inequality. Although many of the examples it gives in the introduction are about how societal inequality increases the likelihood of poor mental health. The few actions that explicitly reference inequalities focus on the unequal way in which people who have mental health problems are treated and how some groups of people with mental health problems such as some minority ethnic communities and people who have been in prison are not treated equally.
Community – Locally the role of community organisations, social prescribing etc is increasingly understood yet the VCS barely scrapes into the report – I spotted one explicit reference with regard to navigators. It is unfortunate that the important contribution that local Healthwatch are increasingly making as positive disruptors in local systems is not affirmed. If there is one area of social policy that needs strong ongoing disruption it is mental health. The need for public and user experience is briefly recognised but needs to be much stronger if real and sustainable change is to occur.
Social Determinants – When the social determinants of health are mentioned it is only within the context of secondary prevention – supported housing and employment support. Of course this is important but we know that the NHS and Social Care are increasingly being used to pick up the fall out from wider government policy attacks on the vulnerable – particularly with regard to changes in the benefit system and housing provision. There is no mention of the prevalence of indebtedness among people with a psychosis despite the strong evidence base to support this.
Money – Others are more expert than me here – but I am not convinced that the £1bn asked for and apparently promised by the Government is close to being sufficient. Tactically the report should at least have called for more funding than it thought the government was likely to give!
What next
- Local Health and Care systems must ensure that the recommendations and focus of this report are understood to be only a small part of the discussion they need to have locally. It is crucial that the role of Housing Providers, Citizens as advocates, Social Care, Employment Support, Access to Education and communities themselves is also included.
- There remains an urgent need for a more holistic mental health strategy that recognises the crucial role of the social determinants of health
What do you think?
Why do vulnerable people need statutory services to help them access their own community?

Personalisation, Social Prescribing and Communities
At the end of last year I was part of a bid that Locality put together to NHS England who were looking to recruit a pool of voluntary organisations who could act as advisors on a call off basis to inform the work of the integrated personal commissioning pilot sites.
We were surprised to be invited to interview, because our impression was that NHSE were looking for voluntary organisations working with particular ‘client groups’. The majority focus on particular client groups as follows:

We felt that a neighbourhood, community centric model might bring added value to this programme – as opposed to the client/condition specific focus of most of the pilots.
The pilot sites are seeking to create a health and care pathway that has the individual at its heart.
I see the logic to this – we are all individuals with our own aspirations, abilities and needs and our circumstances vary. It is important that services bend to our needs and wishes. However, this approach carries with it the cultural heritage and statutory responsibilities of statutory professional services. So, the language includes terms like ‘assessments’, ‘pathways’, ‘reviews’, ‘care plans’.
This model assumes that the first step to support is determined by engagement with the professionals employed by organisations with statutory responsibilities.
Another pathway approach is social prescribing. Many models assume that someone turns up at a GP (one of the champions for this is Dr Michael Dixon), once there an assessment leads to a referral to a ‘broker’ who connects them with a range of community organisations who help address wider issues (such as indebtedness) or help people strengthen social connectedness and regain confidence through doing an activity they enjoy (eg dancing) or giving something back through volunteering.
The difference with this model is the that its focus is on broadening the traditional health and care offer, recognising the important multi-layered contribution that connection with community can have on wellbeing, social determinants and health.
This is all good stuff – however, both of these models are about changing how professional, statutory services behave.
There is a clear need for this…………..but!
Why do vulnerable individuals have to go to statutory service in order to access community and voluntary services where they live?
There is another way in which the same outcomes are achieved and this does not require the initiative to come from health or care professionals.
Community Anchor organisations are a good example of this – many of them are members of Locality. These are organisations like the eponymous Bromley by Bow but they exist all over the country in Sheffield they include Manor and Castle Development Trust, Darnall Wellbeing, SOAR and ShipShape they have roots in neighbourhoods and take a whole person approach – responding to individuals needs and interests but also providing opportunities to contribute, create and get involved.
The way that community anchor organisations work is based on a different set of assumptions. At their best they work to make places better through building services that are run by community members and that are lightly stitched together – responding to the whole person.
Central to this is a recognition that long term relationships are important – community anchors are not going anywhere – they are part of the neighbourhood.
This assumption about relationships and longevity and the more organic way they work; where entry points are many and various is different to the professional model which has clear points of entry, is constrained with regard to the type of services that can be offered and to whom, and relies on professional review and assessment.
At our interview we were not arguing against the professional care pathway – but were saying that there needs to be a balanced approach which recognises the relationship between the professional care pathway and the fuzzier relationships that exist within communities.
It is very important that statutory organisations such as big NHS providers, Clinical Commissioning Groups and those professionals funded by the state like GPs understand that it is not good enough to just design pathways that reconnect people with communities.
Communities are not just waiting with lots of spare capacity for people to be referred to them. They need investment too – the Rotherham Social Prescribing scheme, one of the biggest in the country invests two thirds of its resources in local community and voluntary organisations.
We should support social prescribing and personalisation pathways but commissioners need to give at least as much weight to investing in grass roots community organisations and building their capacity.
What do you think?
Asking or Telling? NHS England Planning Guidance

Interested in localism, citizenship and communities? Then read and take a position on the latest NHS England Planning Guidance. Unlike previous planning guidance although NHS England is calling the shots this is issued jointly with Public Health England, Monitor, Care Quality Commission, Health Education England, NICE and the NHS Trust Development Authority.
This planning guidance follows on from the 5 Year Forward View – which I broadly welcomed here.
Changing Relationships
I think that there is a change of tone compared to the original mandate that NHSE received from Government. We we see a toughening up of Government expectation – with greater direct control and performance management – this is fairly typical behaviour for 2nd term Governments.
At the same time NHSE continue to promote (an albeit imperfect) localism as is shown through their impending devolution of commissioning of General Practice to CCGs.
What I think this means – Simon Stevens continues to push the line that local solutions are the way to address the 3 big challenges highlighted in the guidance (equitable health outcomes, quality of services and financial savings), however, NHSE will be more closely monitored on this approach and held to account (blamed?) if this does not succeed.
Producing local health system Sustainability and Transformation Plans (STPs)
“We are asking every health and care system to come together, to create its own ambitious local blueprint for accelerating its implementation of the Forward View. STPs will be subject to formal assessment”
What I think this means – These proposals seek to accelerate system level action on integration, to some degree they can be read as a belief that Health and Wellbeing Boards have lacked the impetus and capability to do this by themselves.
Those of you who are long in the teeth will remember local Health Improvement Plans (HIMPs) which were a similar intervention brought in by the Labour Government and more recently Joint Health and Wellbeing Strategies – no mention of them in the guidance!
Carrot and Stick
NHSE has to ‘ask’ – it cannot tell local government what to do. However, there are different ways of asking.
“The STPs will become the single application and approval process for being accepted onto programmes with transformational funding for 2017/18 onwards. The most compelling and credible STPs will secure the earliest additional funding from April 2017 onwards”
So this is tough love from NHSE to drive transformation locally. The principles that it sets out with regard to what a STP should involve are hopeful:
“(i) the quality of plans, particularly the scale of ambition and track record of progress already made. The best plans will have a clear and powerful vision. They will create coherence across different elements, for example a prevention plan; self-care and patient empowerment; workforce; digital; new care models; and finance. They will systematically borrow good practice from other geographies, and adopt national frameworks;
(ii) the reach and quality of the local process, including community, voluntary sector and local authority engagement;
(iii) the strength and unity of local system leadership and partnerships, with clear governance structures to deliver them”
Implications
First, NHSE is moving into wider territory seeking to engage with and influence – some might say control areas of social policy that it is not directly responsible for – social care and the broader prevention agenda.
Second, it has set local health and care communities a real challenge – to develop a joint strategic approach that brings together NHS Commissioners, Providers, Local Government and to some degree the VCS. Many of the structures that delivered these have been weakened or dismantled – such as Local Strategic Partnerships. In addition dominant market and Westminster cultures have not fostered the culture and skills to make this sort of local collaboration work. Some Health and Wellbeing Boards are still not mature or inclusive enough to be fit for purpose to respond to this challenge.
Finally, NHSE has a managerial culture and staff establishment that lacks the ability to adequately assess, support and engage with the ambition described here, so there is a real risk that it will fail to establish the processes needed to determine what a good STP is. See my recent experiences of engaging with NHSE here.
Actions
Despite the above caveats I think there is a real opportunity for those of us who believe that if any solution to unmet need, fairer and better services exists in the current policy environment it has to be a local one.
The ambitions require a response from more than the usual suspects. We urgently need to develop local approaches that establish relationships to jointly solve systemic challenges rather than just protect organisations or services this means:
- Coherent approaches to engaging with and supporting citizens who are already or want to be involved in their communities
- Building on the work that some GPs and community anchor organisations have been doing creating neighbourhood services that often have some element of social prescribing.
- Ensuing that the big NHS Trusts are ‘asked’ to engage with this whole system agenda rather than just focussing on the concerns of their own organisation
What do you think?
What do people think about local Healthwatch and why?

At the moment we (Leeds Beckett University) are doing some work for Healthwatch England developing ways in which local Healthwatch and their stakeholders can understand how effective a local Healthwatch is.
It is challenging to come to a view about the effectiveness of a small organisation with a very big remit whose impacts are often long term and therefore hard to measure.
One of the tools we are testing is to gather views of a wide range of local stakeholder organisations through a 360º process using the Healthwatch England Quality Statements (we developed these earlier in the year in partnership with local Healthwatch) to produce an analysis which is then considered at a facilitated workshop.
Gathering and analysing a wider stakeholder view should help contract managers (who are usually middle managers) have a more effective relationship with local Healthwatch.
What is clear is that the opinions of all stakeholders are shaped by the context they work in. Here are some thoughts:
It depends on where you sit
Organisational stakeholder’s perceptions are to some degree influenced by the position and role that they occupy, for example:
- Managers of services may have experienced local Healthwatch through being subject to an investigation or having sight of a report that may relate to their service. So, they will have a good and detailed knowledge of that specific interaction but may not be aware of the broader range of services that local Healthwatch provide or the other roles they perform at a more strategic level. It is also the case that a service that has been investigated by local Healthwatch will have to account for any criticisms they may receive to senior figures in their own organisation – this may feel uncomfortable.
- Leaders such as Cabinet Members, Directors and members of Governing bodies generally have a different experience of local Healthwatch. They are more likely to be aware of the broader scope of Local Healthwatch activities and may have a more personal relationship with local Healthwatch senior officers and board members through formal and informal strategic meetings.
- Different sectors perspectives vary. For example it could be argued that health providers have a view that is focused on the services that they are funded to provide. Local Authorities and NHS providers are large organisations and it is unlikely that all staff will have a shared understanding of a small organisation like Local Healthwatch, while a CCG with fewer staff and a broad health scope may have a more rounded view of local Healthwatch – but within the context of NHS commissioning.
It depends how you talk
There is evidence that the way that large organisations such as local authorities and NHS bodies are organised means that there is an emphasis on understanding the world primarily through analysis of quantitative data (demographic and performance) and evidence from research.
This is not the way in which citizens and communities operate where much more emphasis is placed on personal experience and the stories that describe them. Local Healthwatch operates in between these two constituencies, part of its added value is reflected in its ability to bring the public ‘into the room’ in a way that is understood and accepted by these large organisations.
Remember the history
Local Authorities and many health providers can often trace a continuous history going back over 100 years. It is very easy in the highly pressured environment of health and care to forget that local Healthwatch are actually very small and new organisations. Their effectiveness relies heavily on relationships, with the public and with stakeholder organisations. Local Healthwatch have been in existence for less than three years, they are still developing their expertise and their relationships with citizens and communities.
Moving Forward
So, any analysis of effectiveness cannot just rely on a totting up ratings and opinions – these are important – but there also has to be some account taken of the context that respondents are working within and it needs to be understood that the effectiveness of a local Healthwatch while ultimately its responsibility can be improved by bigger players in the system helping; actions could include:
- Including an explanation of the Healthwatch role in all induction for new staff
- Briefing middle managers on the role and current activities of their local Healthwatch
- Agreeing what good practice should be when working with local Healthwatch on an investigation
What do you think?
With thanks to Healthwatch Dorset and Leicester, the local authorities of Poole, Bournemouth and Dorset and of course, Jennie Chapman
Making the visible invisible – Well North, Public Health England and Health Inequalities

This blog is about the way Public Health England commissioned Well North
To be clear – I am not criticising Aidan Halligan – I am criticising Public Health England – but that will be obvious.
The story
In February 2015 Aidan Halligan a charismatic, passionate and visionary public health champion announced at a conference in Chester that:
“Duncan Selbie has sent me to the North of England to make the invisible visible”
Aidan was announcing the establishment of a programme called ‘Well North’ that was going to support local authorities in the North of England tackle health inequalities. The scheme was to be funded by £9m of Public Health England money over 3 years with the intention of 9 participating local authorities matching this.
Well North (A full description of Well North is available here) with Duncan Selbie as the Board Chair was launched in July 2014
The ideas around Well North built on Aidan’s work on the Homeless Pathway in London, Hot Spot Analysis at Aintree Hospital and high performing teams informed in part by military training methods, the last of which informs some of the ethos of the NHS Staff College where Aidan was the principal.

From Briefing to Oldham Health and Wellbeing Board Alan Higgins Director of Public Health
Like many I was surprised that this initiative had appeared – it had not been publicly requested or tendered for – The Due North Report report (published Sept 2014 and commented on by me here) had been produced by the ‘North coming together’. It makes no mention of ‘Well North’ even though both were in preparation at around the same time and both funded by Public Health England. Yet Duncan Selbie in his Friday Message from 18th of July 2014 which had been endorsed by Felicity Harvey (Department of Health Director General for Public Health) was able to say:
“There is a need to address the causes of ill health as well as seeking to cure the consequences. This has inspired the North to come together in a programme, led by the Academic Health Sciences Centre in Manchester, they are calling Well North, a strategically collaborative programme which seeks to tackle the wider determinant complexity of the whole problem, making visible the previously invisible (predominantly inner city) at risk people and attempting to solve rather than only manage their illnesses and anxieties.”
PHE Management Cttee Paper – Michael Brodie April 2015
A number of people in the Voluntary Sector were irritated – they had been lobbying Public Health England with little success for funding support and suddenly saw £9m go to an initiative that no one seemed to have requested!
A couple of FOI requests later and I was none the wiser.
The report they eventually sent me says that the original idea and approach came from Professor Ian Jacobs, the then Dean of University of Manchester and Director of the Manchester Academic Health Science Centre.
When tragically, Aidan died suddenly and unexpectedly Well North seemed to grind to a halt. It felt as though the whole programme was built around his energy, presence and ideas.
On November 6th 2015 Duncan Selbie in his Friday message told us that:
“Aidan had been the Founder of Well North, he was also the inspiration for its ambitious vision to radically change the life chances of thousands of our citizens who face some of the worst health inequalities in the country.“
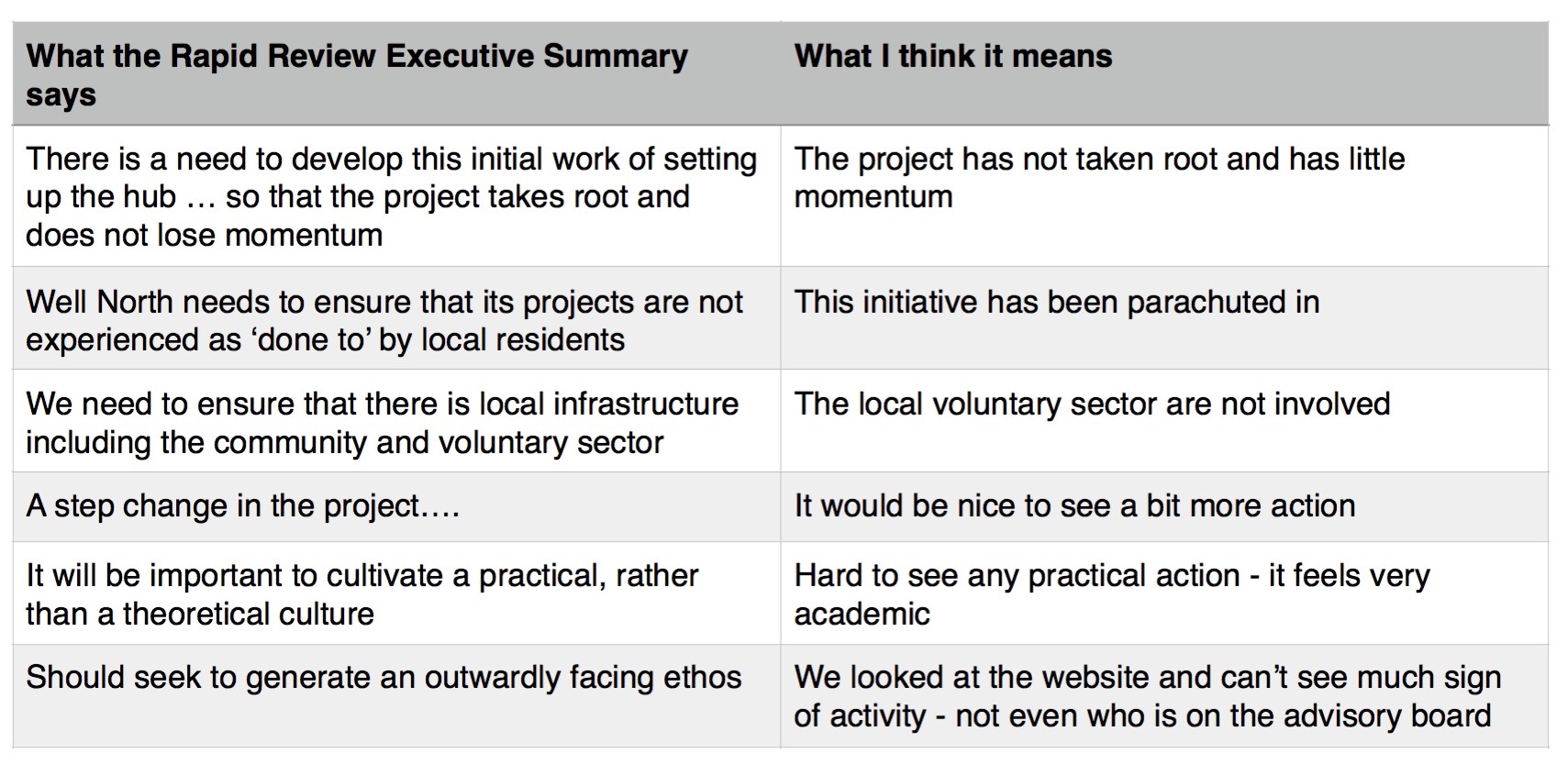
More recently PHE commissioned a Rapid Review of Well North. This has been completed by a team made up of past and present members of Bromley by Bow led by Lord Mawson.
The Review does identify a number of positives – not least the energy and commitment of some of the pilot local authorities. What will be galling to people like Judy Robinson (ex Chief Executive of the sadly missed Involve Yorkshire and Humber – victim of the cuts two months ago) is the emphasis that the review places on shifting resources from the public to voluntary sector, which is a message she and others have consistently championed with PHE.
There are criticisms – if you want an example of how to deliver these diplomatically just read the executive summary – here are some of the key points with my translation.
Lessons
In order to ensure sustainability and impact of any project it is best if:
- Key Stakeholders from the communities concerned are directly involved in identifying what the problem is and have had a role in co-producing the solution
- There is an explicit and public procurement process – not a reliance on ‘who you know’
- The commissioned service is not built around individuals but organisations
- Its always good to make sure that your left hand knows what the right hand is doing
What do you think?
“NHS England will keep you informed” Thats not dialogue!

NHS England has invested millions of pounds in its NHS Citizen programme to strengthen its dialogue with the public. Unfortunately, where it really matters – when its decisions affects whole communities – there is no dialogue.
Here’s the story
Darnall Wellbeing is a small community organisation in Sheffield working alongside citizens in this poor, multi-racial, vibrant part of our city to help them improve their wellbeing. Darnall has a community that includes white British, South Asian, Somali, Roma, Eastern European and more.
Darnall Wellbeing works hard to integrate its services with other voluntary organisations and also the local General Practice – who are all salaried employees of Sheffield Health and Social Care Trust – they are called the Clover Group and provide a General Practice service in 3 other parts of the city as well.
Approximately 3 years ago Darnall Wellbeing made a decision to move into the same premises as the GPs in order to provide a more integrated service. This move is in line with the ambition set out in the NHSE 5 Year Forward View for ‘Multi-Speciality Community Providers’.
This is about providing a better service with citizens from the local community bringing their skills and creativity to create solutions to Health and Wellbeing on their terms.
Darnall Wellbeing has
- 4 Health Trainers (including one recently recruited from the Roma Community)
- Over 40 Volunteer Practice Champions – who work with the General Practice
- Over 40 Community Health Champions
People in Darnall have created:
- Allotments
- Cycle Training
- Dance groups
- Conversation Groups……and more
In addition Darnall Wellbeing is part of the Enhanced Primary and Community Care Project with the General Practice. This identifies those who are most likely to to be at risk of premature hospitalisation and then tailors targeted health and community support to them. The Practice Champions and Heath Trainers are the bridge; building relationships and community support for these priority people.
You can read more about Darnall Wellbeing’s work here.
Then along comes NHS England
NHSE are tendering for the Clover Group service – the outcome will directly affect Darnall Wellbeing and the citizens of Darnall have helped to create this integrated service.
So the chair Dr Jack Czauderna wrote to NHSE on the 9th of October. his letter is available here, one of his key concerns was:
“we are minded about the degree of consultation which NHS England are required to carry out when making commissioning decisions in Primary Care. This particularly applies to the involvement of patients in these decisions. The community organisations, particularly related to Darnall include many Clover patients among their staff and users. DWB has at least 40 Practice Champions who volunteer around health issues but remain patients of the Clover Practice.
We are formally asking you:
- What consultation have you undertaken so far with the communities who rely on these services?
- If asked would you be prepared to come to a public meeting to explain your tender specification and how this will improve the services, assets and health needs of these communities?”
On the 6th of November Darnall Wellbeing received a reply from NHS England NHS England reply (I have taken out names) which can be read here, there is an excerpt below:
“In terms of the consultation process, advice received is that as the services to be recommissioned by NHS England (core, additional and essential GMS services) remain the same. Therefore there is no service change for the element NHS England is responsible for and patients should experience no adverse change to the services they currently receive.
NHS England will be employing a communications strategy to keep patients and the current provider informed of any developments.”
Not good enough
- The ambitions set out in the NHS England five year forward view don’t seem to be understood by staff who are managing procurement. The letter says that services “are the same” as they were before the Five Year View was written. I cannot see how the contract for these services “stays the same” when NHS England has in the interim produced a report that explicitly calls for different service models!
- As I explain above the Darnall service has not “stayed the same’ there are now rich co-produced relationships involving almost 100 local citizen volunteers who are directly involved in delivering a sophisticated holistic service in partnership with the practice.
It feels as though there is a no interest in engaging and talking directly to the communities and organisations who are actively involved in seeking to improve their own wellbeing and are at the front line of creating a the new health service that the five year forward view calls for.
As I said in an earlier blog – I support the 5 year view – its analysis is good and its call for greater integration and strengthening the role of the voluntary sector is spot on its just that NHS England don’t appear to be working to it!
I don’t see how NHS England can run a procurement process without bothering to understand what the Darnall model might be and the implications of this for any tendering process.
What do you think?
Declarations of Interest
I am a trustee of Darnall Wellbeing and a Lay Member on Sheffield Clinical Commissioning Group – the views above do not represent those of either organisation.

Here are 3 small stories about voice and digital. A lot of organisations use digital as a tool to connect with the public. Much of it is ‘broadcasting’ sending messages out, but some also try to to use it enable dialogue and voice.
The first story – can I eat that lettuce?
This story is really just a bit of fun. I was walking past Leeds City Hall and saw that they had turned their flower beds over to vegetables – they looked great! Two people were looking at them and one of them picked a radish to eat and said to me “do you think I am allowed to do this?” I had no idea and tweeted the council with a picture – this is what happened:
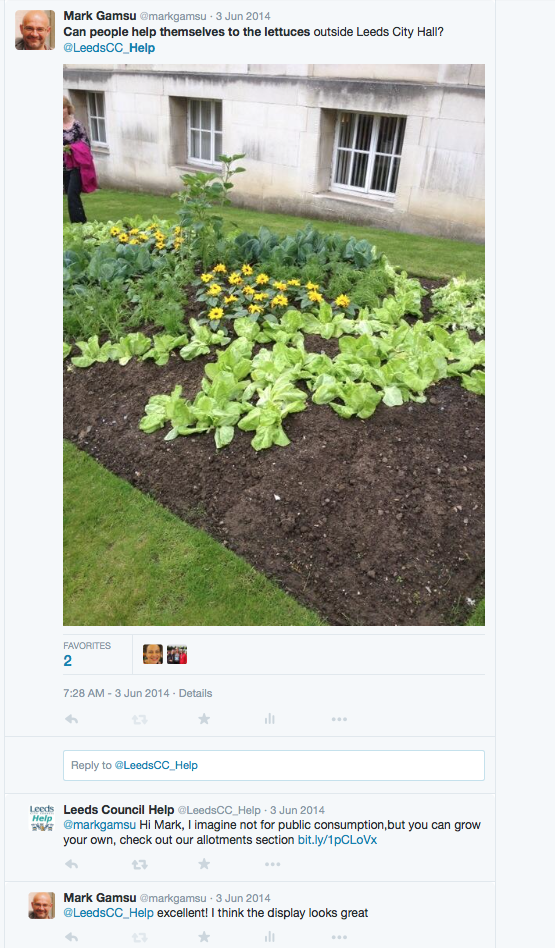
I think the response from the council was great – whoever was managing their account responded quickly, answered the question AND used the request to point me in the direction of their allotment service – clever!
Story two – the Mental Health Champion
Those of you who read this blog regularly will know that I have been involved for years as a trustee of a Citizen Advice Bureau and have a particular interest in improving access to welfare rights for people with mental health problems. I am concerned that there is not consistent provision across the country for this small but vulnerable group of people who are 4 times more likely to be in problematic debt than the general population.
So when Kevin Fenton (National Director for Health and Wellbeing for Public Health England) wrote on his blog saying that he was going to be the organisations champion for mental health I left a comment calling for more action on welfare rights for people with severe mental illness and pointed at the evidence this is what happened:
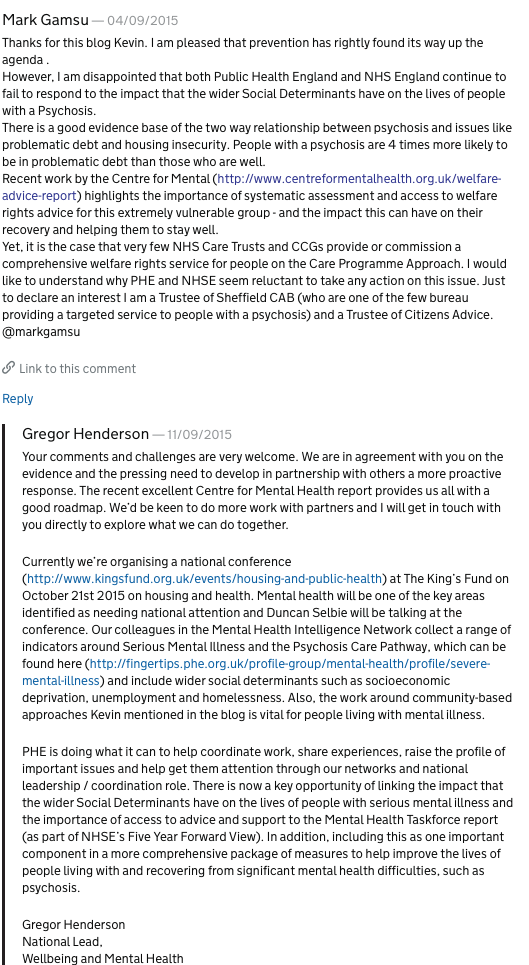
Again, I think the response from PHE was good and since then I have had a conversation with Gregor Henderson and I am hopeful that with the Centre for Mental Health and others we can make some progress on this issue.
Story three – NHS Citizen
One of the ways that twitter is used is to have a ‘tweet chat’ basically a conversation over twitter usually for an hour. So when I spotted that NHS Citizen the engagement arm of NHS England were having a tweet chat on mental health – I joined with the aim of lobbying with regard to the same issue – welfare rights and psychosis. This is what happened:
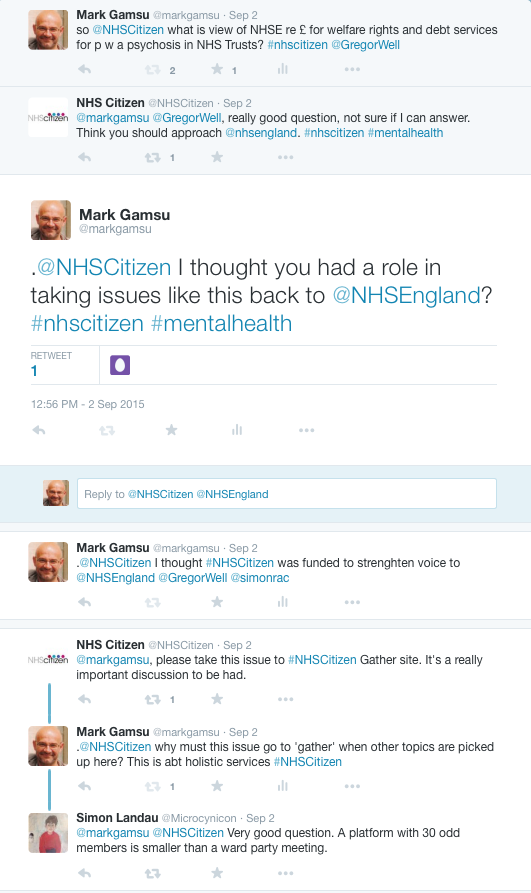
The response here was not so helpful. As you can see the person running the tweet chat referred me to the NHS Citizen portal. As I understand it this is a mechanism that allows members of the public to raise issues – champion them virtually, gather supporters in the hope that by so doing a particular issue will rise to the top and be considered by NHS England at its Assembly.
While in theory this sounds good in practice I am less convinced for a number of reasons:
- It assumes that issues have not already been debated and considered in the real world – so risks adding another layer of bureaucracy
- Surely we don’t need to take all issues through this process – some should be dealt by engaging with appropriate officers
- It makes debate less public taking it into a controlled and managed space – you have to go on to the portal to find out what is going on
- I think it aims to bring a co-produced democratic approach to this sorting – but its a bit of a delusion as it does not attract very many people (see the comment from Simon Landau above) issues are considered by a very small number of digitally literate individuals. Look at the global rank of the NHS Citizen Site (the national engagement website for the NHS) compared to that of a local Clinical Commissioning Group! – not good! Also, see this screenshot taken on the 24th of October 2015 – look at the number of people involved in each issue – the best I found was 70 odd – not in this screenshot.
What this experience made me think about.
NHS England has invested large amounts of money in an extensive ‘digital democracy architecture’, neither Public Health England nor Leeds City Council have – yet my experience with both of these was more productive.
If you are going to have a mechanism for dialogue with the public make sure that:
- the people running the engagement are well informed and using engagement as an opportunity to progress action rather than referring to another place where the member of the public has to start all over again
- the mechanism needs to be simple to use and easy to join
Most fundamentally – theoretically correct and apparently rational models of engagement can actually stifle dialogue and democracy – it should all be more fluid and less managed than this!
There is a broader issue, some private sector companies have a twitter feed that is a key tool for dialogue with the public – from rail companies to Waitrose etc. Public Sector organisations have by and large not gone down this route – there are exceptions like the Leeds City Council example above.
I wonder if NHS England were instead to invest in some empowered staff to manage their public twitter account whether they would actually have much stronger engagement than the complex architecture of NHS Citizen?
Rather than tidying up the dialogue, organisations need to change their behaviour and culture to be more inclusive of the diversity and complexity of conversations
What do you think?
Its not fair! Inequality, the NHS and CCGs

In Sheffield some of us met recently to wrestle with what a Clinical Commissioning Group (CCG) health inequalities strategy should look like.
At the moment this is still very much a discussion rather than a strategy or policy – however, I think that some useful insights are beginning to emerge.
We thought that there are potentially three areas of focus that a Clinical Commissioning Group should be considering, these are:
Membership
As we move towards ‘co-commissioning’ of primary care it becomes even more important to consider what the roles of primary care and General Practice specifically should be in a local health system. This means building on the strengths that the General Practitioner membership of CCGs brings. This could include:
- developing closer partnerships with community organisations to help address the social determinants of health
- using social prescribing systematically
- consistent use of practice champions to create pathways of support and connection
There might also be a need to work with the CCG membership to develop a shared view of what we understand health inequalities to be – this is because it does still feel that people hold different views about what words like inequality and equality mean. For example sometimes conflating a focus on ‘protected characteristics’ with work on health inequality.
Regrettably there is also a minority within the medical profession who still find it too easy to blame the poor for their ill health – as a generally dispiriting list of comments from in response an article in Pulse about food banks shows – these views need to be challenged.
Commissioning
This is of course the official role of Clinical Commissioning Groups however more needs to be done, for example:
- How do CCGs ensure that big NHS providers in particular take a clear responsibility for ensuring that that their services respond to the needs of people with multiple disadvantage? There is a real issue of people failing to engage with secondary services because of their complexity, language and cultural barriers and issues like access to transport.
- What can CCGs do to ensure that big NHS providers have a coherent health inequalities strategy that goes further than a focus on protected characteristics and HR policy?
- We need to avoid tackling health inequalities being seen as something that is done through small stand alone procurement exercises.
System Leadership
The third strand is the CCGs relationship with the wider local health system. This includes a wide range of issues – but particularly connection through the Health and Wellbeing Board with work to address the Social Determinants of Health. So here we might expect to see connections with:
- Strategic work on voluntary sector and volunteer development
- Work on income, debt and poverty
- Strategic work on voice and advocacy
It could also mean considering the relationship that a CCG Health Inequalities Strategy has to key local plans such as priorities that might emerge from Fairness Commissions – where these have been carried out.
What do you think?
I would be very interested in ideas and approaches from other CCGs who are trying to take a more strategic approach here.
With thanks to Susan Hird, Leigh Sorsbie and Ted Turner
