Act on health inequalities? Learn from the past
I was recently asked to give a talk about Health Inequality and as part of it I dug out a graph that I used to use a lot when I worked for the Department of Health.
The graph shows the widening mortality gap for working age men over the last 75 years or so – it compares the top social class (I) with the bottom one (V). It starts in the 1930’s and ends in the 1990’s – I would be interested to know if there is a more up to date version.
Ever since I came across this graph I have been intrigued by it. This is because I think we take an ahistorical approach to tackling inequality. In part this is because every government that comes in seems to assume that we are at year zero – witness Teresa May’s address from the steps of Downing Street when she took office, but its also because most programmes and actions assume a three to five year timespan – and as the graph shows tackling health inequalities is not a 3 or 5 year project.
So lets have a look at the graph – bear in mind that the graph is comparing the gap in mortality rates for men of working age – comparing social class I (bottom line) with social class V (top line). Note there is no data for 1981 because there was a local registry officer strike that year and no records were kept.

As you can see while the mortality rates for both groups goes down – it goes down far quicker for men in social class I compared to social class V.
Here are some things that stand out for me.
- Prior to the war the gap in mortality rates is fairly narrow and pretty stable. I assume that this is because infectious disease like TB did not discriminate between social class. Nonetheless the narrowness of this gap does surprise me.
- It is after the second World War that the size of the gap really starts to grow, and it does not really stop growing. This is a bit difficult for those of us who are supporters of the NHS – because this is when the NHS was created!
- Of course it could be that without the NHS the gap might have grown faster and been even bigger; or that the NHS had no effect at all or even worse that the NHS is one of the reasons for the growth in the gap! I have toyed around with whether this might be due in part to Tudor Harts inverse care law. However, we are talking about comparisons between social classes V so I am less convinced about this.
- I have wondered whether the size of the gap is in part due to other elements of the post war social contract – such as the increased social mobility bought about by improvements in access to Higher Education.
- When I spoke about this with Chris Bentley (albeit in the pub!) – who was head of the Department of Health; Health Inequalities National Support Team he reckoned it was because the combination of socio-economic disadvantage and burden of disease in Class V since the second world war and onwards meant that many working age men in that group just did not have the wherewithal to keep pace with Social Class I. He particularly mentioned smoking – and the failure of respective government’s to reduce smoking rates among the most disadvantaged at the same rate as for wealthier people.
Why this is relevant now
We are in a very difficult period of government imposed austerity. The Health Inequalities gap appears to be widening – in part because the safety net provided by the state is increasingly threadbare – we see the NHS struggling to provide a consistent and accessible service, adult social care experiencing huge cuts and welfare support diminishing – as is set out in the report by Joseph Rowntree and Dominic Harrison DPH for Blackburn. For me the lesson this graph tells us is that we need to be much better at recognising all of the systemic drivers – not just the NHS – and defending those.
By the way the answer is clearly not more targeted anti-smoking leaflets at the most worse off!
What do you think?
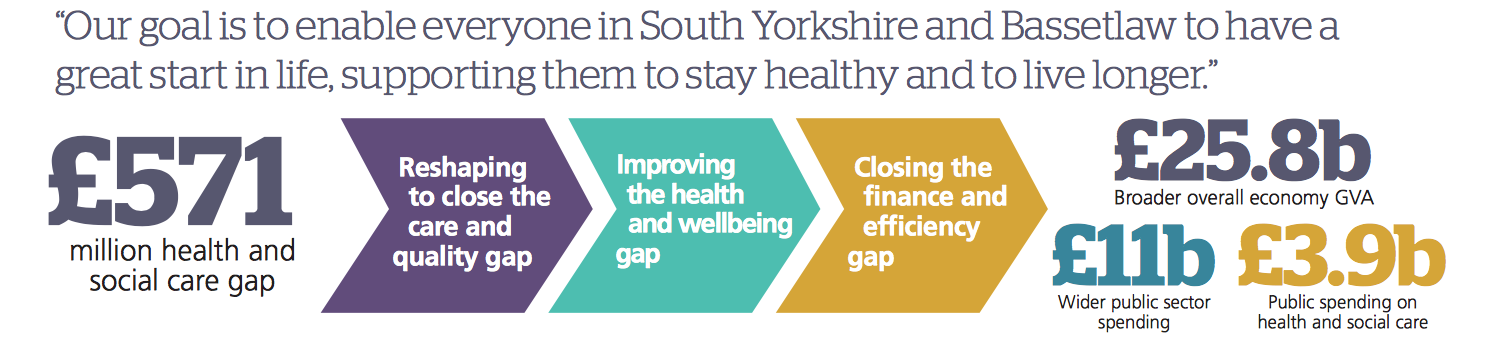
Who is afraid of the big bad Sustainability and Transformation Plan?

In South Yorkshire and Bassetlaw we are busy thinking about the next phase of discussion on our Sustainability and Transformation Plan (STP). There is a useful and serious group of CCG engagement leads, the voluntary sector and local Healthwatch who are collaborating on developing a shared approach to deepening discussion with the public this year.
These discussions have led me to revisit our STP a number of times – simply because I cannot retain in my mind what it says the problem is and what it is trying to achieve.
I now think that my difficulty in grasping this is only in part due to my failing memory and limited intelligence- its also to do with the fact that STPs claim to be something that they are not.
I think that STPs are represented as THE overarching strategic plan for sub-regional health systems. However, if we look closely at them – the actions that stand out relate to plans to make specific NHS services – usually hospital based more effective and (hopefully) more efficient. There is nothing particularly threatening or wrong about this – in a number of cases these plans existed before STPs were thought of.
Of course STPs also try describe a wider vision and set of principles for local health systems – care closer to home, greater emphasis on prevention, tackling inequality etc. Here the actions are not clear – largely because STPs are NHS documents and this is a world where the NHS has less responsibility and influence. Again, nothing particularly new here – we have been concerned about these issues for some time …. and failed to make a great deal of progress.
The theory is that STPs will join these two issues up – greater efficiencies in hospital care will lead to greater investment in community, prevention etc – its an optimistic scenario.
Trusting STPs.
Its difficult to have faith in a plan that many people believe is primarily concerned with implementing cuts to health systems. In my experience STPs represent the projected funding shortfall (in South Yorkshire and Bassetlaw this is some £571 million) as being due to rising demand and inefficiency – when we know it is largely due to a government policy decision to restrict NHS funding and cut funding to local government.
Second, STPs run the risk of assuming that the NHS can produce plans that will of themselves solve societal and socio-economic problems.
Many of the heath and wellbeing problems that people face are caused by factors that have nothing to do with the NHS – poor quality employment, reduction in social welfare support, low wages, cuts in adult social care etc. All of these create demand on one of the few parts of the public sector that has been relatively protected and is not rationed – the NHS.
There is a real danger that if we are not clear about the actual challenges facing the health and well being of the population and why these impact on the NHS that we will have a distorted discussion about the future shape and role of NHS services.
Three things we need to do:
First – lets be honest about:
- the state of funding of the NHS – it is under pressure due to government cuts,
- where the cost pressures actually come from – for example we need to include the impact of cuts in social welfare support services and adult social care
- how much healthcare costs us in England compared to other equivalent western economies – the NHS is still one of the cheapest healthcare systems – we MUST always present this evidence to members of the public.
Second – local discussions must start from peoples experience of what health and wellbeing means to them. We have to talk about the whole experience here not just the NHS bit. Our starting point should be the whole journey not specific services such as General Practice. For example in an earlier blog I wrote about a video I had helped produce about a man who received excellent treatment in hospital for his stroke – but was then left on his own to cope with – social isolation, physical disability, lack of role, access to benefits – not surprising he became depressed and needed help from a range of NHS services that he should never have needed in the first place.
Finally – Lets be honest about what STPs can realistically achieve – otherwise we risk people feeling threatened and anxious about what they claim to be – seeing a lack of detail as an indication of secrecy rather than what it actually is – a collection of practical plans to improve hospital services and some rather vague ambitions to contribute to the development of a more integrated health and care system.
I am more hopeful about the “place based plans” which in theory underpin STPs. In Sheffield’s case they are Shaping Sheffield and sister documents such as the Primary Care Strategy These come much closer to joining up community and prevention, not least because they have a stronger connection with local government – albeit one that still needs further development.
What do you think?
Through a glass darkly – inequalities, public health and NHS data on mental health

The NHS 5 Year Forward View gives a clear call for a re-balanced approach to prevention, clinical services, and community support and notes how important this is to help us tackle health inequalities and poor mental health.
But….those of those who are involved locally know that its all very well having the analysis and the aspiration – translating this into action is something else.
I want to focus on how our use of data shapes our approach to mental health and how this determines what we commission and provide – I think that this tends to leads us in one direction only – towards clinical solutions for social problems. We can see this in the report of the Independent Task Force on Mental Health to the NHS in England – although it recognises poverty as a significant driver for poor mental health its focus on inequalities is almost exclusively on ensuring equal access to clinical services – not on the social circumstances in which people with mental health problems live..
Lets look at the national data – because these set the tone for how we use data locally.
Problem One
The Public Health England Public Health Profiles do include mental health indicators – but they only have two. These are for quite specific issues – incidence of suicide and deaths from drug misuse. There is nothing on broader issues such as anxiety and depression.
Problem Two
We know about the relationship between poor mental health – anxiety, depression and inequalities but most of the measures that pick up on inequality in the Public Health Profiles do so at a county/borough/city level – so the extent of inequality is masked by those who are better off.
Problem Three
There are more detailed mental health indicators that are produced by Public Health England. Two that are particularly helpful are the Common Mental Health Disorders and the Severe Mental Illness Profiles.
There is a tremendous amount of detail in both of these – with an overwhelming emphasis on data from statutory clinical health services. However once again they fail to locate the incidence of anxiety and depression within the wider socio-economic context of a particular district. There is a section on ‘Risk Factors’ which is deprivation related. But I think that the scale of the issue here is masked by a wider population effect.
Problem Four
As I have said almost all the data in the mental health datasets looks at the performance of the Health and Care mental health system. This means that there is a constant pull back towards clinical interventions.
Yet as the APHO 2007 report “indications-of-public-health-in-the-english-regions-7-mental-health” notes we need to focus on the needs of those who experience inequality most – this means focussing on:
- Housing Insecurity
- Problematic Debt
- Low wage and insecure employment
- Take up of welfare rights support
- Social Isolation
While some of this data sit in a background document to the Mental Health profiles (cmhd indicator list v5 march-2016) each indicator is presented in isolation and so does not give a coherent picture of the negative social factors that people with mental health problems experience.
This failure to present a coherent narrative about the relationship between mental health and inequality means that local health and care systems lack the evidence that will help them make the significant changes that are needed to rebalance services to focus more on prevention and community support.
What needs to happen
- PHE and NHS England need to start to produce a data set that describes the scale of the risk factors that are faced by populations of people with poor mental health AND data sets that focus on the risk factors faced by people in the bottom 20% of the population by income – compared to those in the top 20%
- More work needs to be done to bring key voluntary sector data into these profiles. There is plenty of data out there – for example voluntary sector and social landlords have good data on housing insecurity, Citizens Advice and Stepchange have excellent data on incidence of indebtedness and so on.
The recent report “The Missing Link” from the Money and Mental Health Policy Institute notes that:
“The IAPT recovery rate for people experiencing both depression and financial difficulty is likely to be just 22%, compared to 55% for people without financial difficulties. For anxiety, the IAPT recovery rate is likely to be just 38% among those with financial difficulties, while over half of patients without financial difficulties recover through IAPT.
We found that an intervention on financial difficulty boosts the likelihood of recovery for an individual with depression and financial difficulties from 22% to 48% and for an individual with anxiety and financial difficulties the likelihood of recovery increases from 38% to 50%.
What do you think?
The confusing world of NHS patient feedback
Over the last ten years or so there has been a huge rise in ways in which members of the public can give feedback about their experience of health and care services. This information is one of the ways in which service providers such as hospital trusts, as well as commissioners of these services can get an insight into the quality of services and what needs to improve.
These days there are a range of channels through which people can leave feedback about their experience. These have a variety of purposes:
- Complimenting or complaining about a particular service or experience that will help a service improve.
- Giving a rating that helps other potential service users to decide whether or not to use a particular service
- Creating a dialogue between a ‘customer’ and a provider which might help resolve a problem and build a relationship
- Giving commissioners an insight into how a service is performing through looking at public feedback in the round and comparing this against others.
I think there are 3 main ways in which the opinions and views of people are captured. Some of these rely on the public taking the first step and others reach out to the public.
- Provider organisations all have some way to capture comments and complaints from individuals. These are are specific to the organisation and rely on individual members of the public finding their way to them – they include in house complaints, Friends and Family, PALS services etc.
- Another channel that relies on the public finding their way to them are specialist or stand alone feedback organisations or services such as Care Opinion, Healthwatch Rate and Review (this is NOT a Healthwatch England initiative, but used by some local Healthwatch) and NHS Choices – these rely on their own publicity or commissioners/providers promoting them.
- Then there are National and Local Surveys that pro-actively reach out to the public and try capture a representative sample of peoples experiences of particular services. These may be useful at a national level but their sample sizes are often quite small at a provider level.
Of course it is not quite as neat and tidy as this – for example Friends and Family is provided at an organisation or service level but there is an expectation that providers will pro-actively encourage people to use it.
Different approaches different insights
The situation is further complicated because these mechanisms vary:
Most are service specific – in that they are based on the experience of using a specific service – or even more narrowly the experience of using a service on a particular occasion.
The one that is probably most sophisticated and different is Patient Opinion which starts in a different place – it asks people to tell the story of their issue and from this constructs and connects with various services who may be able to respond.
Care Opinion is interesting because it tries to respond to the whole person rather than just treating someone as though they are the sum of their condition. I think this is particularly important given that local health systems are increasingly trying to develop more integrated and personalised services.
The situation is further complicated by how well signposted feedback services are. Here are examples with web links from three NHS Trusts.
Guys and St Thomas NHS Foundation Trust
This is one click from the main page of the website by clicking on the tab that says ‘your feedback’ one gets access to a range of internal feedback mechanisms.
This is also one click from the main page but a bit harder to find – its on a tab saying ‘Contact Us’ and the feedback form comes after some more administrative information.
Northumbria NHS Foundation Trust
Here the link to feedback is shouting out on the main page – although a bit confusing there are then links to internal complaints, comments and advice on how to get in touch with advocacy services.
None of the above organisations appeared to promote independent channels such as Care Opinion or Healthwatch Rate and Review.
Issues
I think that there is inconsistency with regard to how feedback mechanisms are used across the health system. With different channels of varying utility and a wide variation in terms of how they are promoted. For example the government suggests a variety of ways in which Friends and Family information can be collected:
- There are few constraints on the technology used to collect the data, and a number of different methods would be suitable, for example:
- On-line rating: patients are given information including a web link which they can use to log on, enter a reference number and provide their feedback
- SMS/Text message: patients are given the question at the point of discharge, and are able to text their response (providing an opportunity to send follow-up questions to responders)
- Smart phone apps: patients are given details of the app, including a unique reference number, at the point of discharge
- ‘Voting booth’ kiosks or hand held devices: positioned in the location from which the patient is discharged, with ‘voting’ controlled to allow each patient to only vote once
- Telephone survey – patient is given a freephone number and a unique respondent ID to respond within 48 hours
- Postcard solutions: patients are given a postcard at discharge with an option to complete and return on site or to complete at home and post back.
This variation and the range of different feedback channels makes it harder for the public to decide which one to use and more difficult for providers and commissioners to assess the overall picture of public opinion about services.
It’s interesting that Healthwatch have now entered this area with ‘Rate and Review’. While the logic of this is clear – it brings a systematic way for them and CQC to keep in touch with public concerns it also raises more fundamental questions – in particular how they get the balance between being the provider of a feedback channel at the same time as being responsible for stress testing whether or not a system offers adequate and consistent opportunities for feedback.
I do think that there needs to be some thoughtful work done to consider what good might look like and the respective merits of different feedback systems to ensure that we don’t just gather feedback on individual experience but capture this in a way that helps us to develop more integrated local systems.
What do you think?
Nudge, Nudge, Public Health England and Behaviour Change
“Welcome back Trevor! – As Trevor Hopkins says below following his comment on my recent blog I suggested he might like me to post these as a full blog. Instead he has developed some of his arguments about Public Health England and Nudge. My personal view is that the emphasis on behavioural insights is not as strong or as self consciously planned in Public Health England as the article below might lead some to think and that behavioural insight approaches are not as powerful as we might fear. Nonetheless I think as always Trevor’s arguments are worth reading – if only so that we can be clearer about our own analysis – so read on!”
Mark Gamsu

As a guest blogger can I thank Mark for this opportunity to further explore some of the issues that I raised in my recent reply to Mark’s blog ‘Public Health England, Health Trainers and Health Inequalities’.
In my reply to Mark’s excellent piece I stated that I was not surprised, “when a charity can produce a more coherent narrative on behaviour change than the government’s leading Public Health agency.” I laid much of this on PHE’s lack of a “coherent or up to date” theory of public health. As long ago as 1996 in his book, ‘Health Promotion: Philosophy, Prejudice and Practice’. Professor David Seedhouse famously described public health as a ‘magpie profession’ lacking a consistent theory for their approaches. As you observe in your blog the latest glinting object they have picked up seems to be the ‘behavioural insights’ approach.
The recent LGA publication ‘Behavioural insights and health’ (2016) traces the history of where this comes from,
“Much of the interest in behavioural insights on a policy level stems from the 2008 book ‘Nudge: Improving Decisions about Health, Wealth and Happiness’ which was written by US academics Richard Thaler and Cass Sunstein.”
It has both the look and the witty approach of one of those books on DIY personal improvement you see in airport bookshops.
“Though costumed in the guise of pop economics, complete with a cute logo – Nudge is, in fact, a manifesto for the new paternalism… don’t be fooled. Thaler and Sunstein charm their readers but they are after some very big game. This is a book that measures both the inroads psychology has made into contemporary economics, and argues a compelling brief for the new paternalism. We have ways, say Thaler and Sunstein, of making you happy!”
(from a review by Thomas C Leonard, Department of Economics, Princeton University, published online by Springer in 2008)
Behavioural insights really came to the forefront of government policy though when the coalition was formed in 2010. In fact, the coalition agreement itself made direct reference to the issue, stating that the government would be “harnessing the insights from behavioural economics and social psychology.” So this is quite clearly a Politically (with a big P) driven agenda – some would say, myself included, it looks more like ‘policy driven evidence’ than ‘evidence led practice’. The theory that “libertarianism and paternalism do not have to conflict and that the state can – and should – act as a guiding hand, ‘nudging’ citizens in the right direction.” (LGA – ibid) is highly insidious. Gone is the ineffective old-fashioned finger wagging approach to health behaviour change, in comes state sponsored behaviour change interventions that we will probably be unaware of and certainly, unlike other medical interventions, have not given our consent for.
Perhaps the biggest give-away that this is a Politically driven dogma, possibly an example of lax editing, comes in the 2010 Cabinet Office discussion paper ‘Applying behavioural insight to health’ (forward by Conservative MP Oliver Letwin) which states “The Behavioural Insights Team would like to thank in particular Department of Health Ministers and officials, whose expertise and support were vital.”
So what is ‘dispiriting’ you and me Mark is an ostensibly ’arms length’ PHE resourcing and implementing a paternalistic libertarian approach to health improvement driven by the Behavioural Insights Team based on nudge theory and clearly supported by senior Tory politicians and Civil Servants.
For Foucault the bigger problem is that this is all “predicated on our societal regime of truth, the types of discourse it accepts and makes function as true; the mechanisms and instances that enable one to distinguish true and false statements; the means by which each is sanctioned; the techniques and procedures accorded value in the acquisition of truth; the status of those who are charged with saying what counts as true.” It seems to me that PHE are making all the claims to the ‘the truth’ while ordinary people and communities remain marginalised or ignored in this discourse. In my previous reply I noted that supporters of a fifth wave of public health cited truth as a key issue in their new paradigm.
I will finish with some thoughts from my favourite post-structuralist philosopher and social theorist Michel Foucault that the truth is characterised by important traits, “It is centred on the form of scientific discourse and the institutions that produce it; it is subject to constant economic and political incitement; it is produced and transmitted under the control, dominant if not exclusive, of a few great political and economic apparatuses; finally it is the issue of a whole political debate and social confrontation.” (from an interview conducted in 1976)
To mark his death in 2002 the Journal of Epidemiological Community Health reproduced an article on Ivan Illich’s famous publication ‘Medical Nemesis’ first published in a 1974 issue of the medical profession’s house magazine The Lancet. It contained the following:
“The level of public health corresponds to the degree to which the means and responsibility for coping with illness are distributed amongst the total population. This ability to cope can be enhanced but never replaced by medical intervention in the lives of people or the hygienic characteristics of the environment. That society which can reduce professional intervention to the minimum will provide the best conditions for health. The greater the potential for autonomous adaptation to self and to others and to the environment, the less management of adaptation will be needed or tolerated.”
What do you think?

Recently I was lucky enough to speak at the the annual Health Trainer conference organised by the Royal Society of Public Health. All credit to the RSPH who have been steadfast in their support for this service, building on the early work from Leeds Beckett University – in particular my colleague Judy White.
Around since 2004
Health Trainers have had remarkable staying power – here is a bit of history from the Health Trainers England website:
The role of health trainer was first outlined in the 2004 White paper Choosing Health. Since their inception they have generated a great deal of interest from commissioners, provider services and the public. From the start they were intended to offer support from next door rather than advice from on high and their aim was to:
- Target ‘hard to reach’ and disadvantaged groups
- Increase healthy behaviour and uptake of preventative serviceProvide opportunities for people from disadvantaged backgrounds to gain skills and employment
- Reduce health inequalities
The different approach taken by two of the key speakers at the conference unintentionally highlighted some of the tensions that exist with regard to Health Trainers. This tension is set out in a good report (Indicators of Change – the adaptation of the health trainer service in England) produced by Emma Lloyd the Policy and Research Executive for the RSPH
In the paper Emma notes that:
“There is a growing polarisation of services, between on the one hand services adopting more clinical work and on the other services consciously resisting this move and instead, placing a far greater focus on the wider determinants of health and community development”
Clinical Model
The first major presentation was from Kevin Fenton who is the National Director for Health and Wellbeing at the government agency Public Health England
If I understood him correctly his presentation focussed on the way in which the evidence base has developed – and the opportunities that are presented by bringing ‘behavioural insight theory’ which is to some significant degree informed by the work of the Behavioural Insights Team – formerly the Cabinet Office Nudge Unit.
The presentation dispirited me – it highlighted the disconnect between Public Health England and the experience of citizens – particularly the most disadvantaged. There was no mention of health inequalities at all and little understanding shown about the connections that exist between poor mental health and vulnerability. Instead we had the usual rather technocratic sets of interventions targeted at particular behaviours (smoking) or conditions (obesity). It felt as though Public Health England are trying to shoehorn Health Trainers into an older clinical model of behaviour change – the person as a collection of conditions.
Social Model
The second presentation was completely different. It was by Sam German – who is supporting an initiative called called The Healthy Villages Partnership. He told us stories of connection and relationships. For example a story of an elderly woman who was isolated and depressed following the death of her husband and how a community health worker helped her reconnect with one of her passions – dancing – and the difference this made to her health and wellbeing.
The key for me was that people – their circumstances, histories AND skills and hopes were at the centre of Sam’s narrative.
I find this dissonance between these two views quite shocking. One is about ‘the other’ as though we are a just a collection of behaviours to be triggered and the other is about seeing us as human beings who want to be creative, who want to give and whose circumstances are one of the things we have to recognise and address if we are to be fulfilled.
Coincidentally at around the same time as this conference Citizens Advice produced a report in association with the Behavioural Insights Team called “Applying behavioural Insights to regulated markets” which looks at how behaviour change theory can help people take control as consumers of financial and utility services. Unlike the Public Health England presentation it does recognise the impact of inequality and vulnerability on our ability to change our behaviour and take control.
What needs to happen.
- Public Health England need to change their paradigm. At the moment they produce too much material that feels disconnected from the lived experience of people – they urgently need to develop a whole person narrative rather than a condition focussed one.
- PHE must raise their game with regard to the science – it is frankly embarrassing when a charity can produce a more coherent narrative on behaviour change than the governments leading Public Health agency.
- We urgently need an assertive position on the person centred role of health trainers, health champions or community health workers that affirms the importance of this approach to counterbalance the a-contextual science of the Public Health England model.
What do you think?
Private Sector Health Providers and local accountability – Quality Accounts and local Healthwatch

In an earlier blog I mentioned some of the good practice being developed by local Healthwatch with regard to engaging with and influencing Quality Accounts.
The NHS Choices website states that there is a statutory responsibility for all healthcare providers over a certain size to produce a Quality Account and to seek the views of local Healthwatch who if they wish may send a written response. This is affirmed in the Healthwatch England Guidance.
The logic is clear – a bit of local voice based on the experience of the public can provide a reality check, foster engagement and bring a bit of informed challenge to this annual statement.
This mechanism could become more important as we move to more devolution, integrated care and co-production with the public as local health and care systems respond to the ambitions set out in the Five Year Forward View.
Whats the problem?
When we compare the approach taken by NHS Trusts to the private sector in particular there is a striking contrast. While the private sector does produce Quality Accounts their quality is more variable and they often do not appear to seek the views of local Healthwatch or the local Overview and Scrutiny Committee.
A quick scan of a couple of private hospitals in Sheffield shows that only one mentions engagement with their local Healthwatch.
- Thornbury Hospital Quality Account – no mention
- Claremont Hospital Quality Account – asked for comments
The problem gets worse when you look at some of the big players in this field who operate across the country.
For example Partnerships in Care have around 60 sites across the country and specialise in providing services to some of the most vulnerable people (people with a learning disability, people with a head injury and people with a mental health problem). They produce one Quality Account for the whole service and it has no comment from a Healthwatch – although it does have a comment from one ex service user who now works for Rethink he also commented in the previous Quality Account.
Service user comments are very important – and a number of private sector Quality Accounts have these – however, I think the views of an organisation such as a local Healthwatch are qualitatively different – they have a duty to consider a Quality Account when asked and are accountable for the views they express in a way that individuals are not, in the case above I don’t think that the comment reflects the views of Rethink.
I could not find many examples of where a private sector provider has sought the views of a local Healthwatch and that Healthwatch has responded – but there are some.
Care UK in their 2014/15 Quality Account include comments from Healthwatch in South Gloucestershire and in Bristol. Also since writing the blog Sian Balsom from Healthwatch York has said that the Ramsay Clifton Park Hospital in York have asked them to comment on their Quality Account for the last two years. However, Ramsay have a network of 22 acute hospitals and their practice does vary – for example there is no mention of Healthwatch in the Ramsay Berkshire Independent Hospital Quality Account.
I could find no mention of local Healthwatch in the Quality Accounts that I looked at from:
Circle Group – for example see Bath and Nottingham
BMI General Healthcare – see for example the Priory Hospital Birmingham and Clementine Hospital
Spire Healthcare produce a national Quality Account – again no mention of Healthwatch in their Quality Accounts
Priory Group who are an acute mental health provider – who also produce one Quality Account
This national issue does not just apply to private sector providers – have a look at the one produced by Marie Stopes – again no mention of local Healthwatch.
Where this leaves us
Advice from NHS Choices is as follows

There is considerable variation with regard to how independent providers use Quality Accounts and what they expect from them. It does seem as though many independent providers are working in a parallel world where they have a much narrower view of the purpose of Quality Accounts and their relationship with local Healthwatch than NHS Trusts.
- Some big national independents produce one Quality Account for all their sites.
- Others produce a quality account for each site.
- A minority seek the views of local Healthwatch – most don’t appear to.
- There is a wide variation in the quality and accessibility of the Quality Accounts produced.
What should be done?
- Local Healthwatch with the support of Healthwatch England should develop an explicit strategy for engaging with the Quality Accounts of the big national providers.
- Clinical Commissioning Groups should take a more robust approach to challenging private sector providers on the content and quality of their Quality Accounts – some of the ones I looked at above are inaccessible and uninspired.
- Finally, I think that NHS Improvement need to produce some clear guidance for non NHS providers stating clearly why producing accessible and engaging Quality Accounts is important and why local Healthwatch must be involved in commenting on them.
What do you think?

I recently attended a discussion organised by the Galileo Group which considered the above question.
The title comes from a statement by Conservative peer Lord Hodgson, a member of the All-Party Parliamentary Group on Charities and Volunteering, who stated ‘what planet are these people on’? When he heard that one of the largest charities did not want to pay £15,000 to set up the new Fundraising Regulator.
Since this discussion the Charity Commission Report “Public Trust and Confidence in Charities” notes that the level of trust and confidence in charities has fallen to 5.7/10 compared to 6.7/10 in 2012 and 2014.
The temptation is for the Charity Sector to accept the analysis of Lord Hodgson and of the Charity Commission and focus inwards on improvement. I am not convinced that there is any evidence that the sector as a whole has witnessed a deterioration in standards of practice.
Instead I think we are experiencing a ‘moral panic’ driven by an unpleasant mixture of government, some think tanks and some elements of the press
The sector is being criticised in a number of ways:
- its independence and legitimacy to campaign
- the strategies they use to fundraise
- the competence of its governance
There have been cases where some charities have not been as good as we have the right to expect. However, I see no evidence that the current performance of the charitable sector is any worse now than it has been in the past. In fact the growth of an executive function and the diminution of the role of trustees has ironically probably led to greater organisational competence.
It is therefore disappointing when organisations like the Charity Commission fail to provide wider evidence of the competence of the sector and instead produce reports which tell us that the public have lost confidence in the sector because the media and government tell them that the sector is behaving badly.
If you look at other sectors (Banking – various miselling scandals), Service Sector (G4S, SERCO, A4E), High Street Retail (BHS etc), NHS Trusts (Mid Staffs) and judge them on the above criteria there are much stronger grounds for being concerned about their legitimacy, fundraising strategies and governance rather than that of big national charities.
I think that the current highly critical environment exists (there is a good summary in the Morning Star here) – not because the sector is failing – rather the reverse – its actually rather successful despite government imposed austerity. I think this relative success exposes the national voluntary sector to attack because there is:
- dislike of independent challenge to government
- concern that the charity model of service delivery is a direct challenge to that offered by private sector corporates who are fishing in the same pond for government contracts.
- belief that large charities are a redoubt of the left of centre professional class
Sympathy
I have some sympathy for national charities (I am on the board of one – Citizens Advice) they have responded to the marketisation of public sector funding and the move away from grant funding – in some cases quite successfully. This must be galling to private sector providers who are keen to get access to the lucrative public sector market.
Action
I think that the sector needs to develop a more strategic response here.
- Evidence – there needs to be a clear evidence based view of the competence of the sector. If the Charity Commission cannot do this (and in my view it should) then other players like NCVO need to step up and do the work – we urgently need a robust and clear view of the sector which challenges this moral panic.
- Governance – it is too easy to portray many charities as the mouthpiece of the professional ‘charitariat’, it may feel frustrating for some to to give some power over to members and trustees but strong accountability and roots into the communities we serve is essential to charities survival and is an important way of keeping true to founding values – avoiding a drift to social enterprise or business.
- Challenge – national charities must see the gagging legislation as giving them a mandate for evidence based challenge rather than a restriction. Part of all charities business plans should be to raise funds to ensure that they can lobby appropriately to represent the interests of the people who rely on their services.
- Government – finally the sector should have the confidence to challenge government. A number of the problems here rest with government behaviour. From the sweetheart deals that were done by ministers with Kids Company, through to the way in which lobbying from some charities and private sector companies is condoned while charities are attacked – we need a coherent challenge that places these issues in the wider context of policy influence and access to markets.
What do you think?

Remember the Department of Health Responsibility Deal? It emerged in the early days of the Coalition Government, well, I think its gone. I cannot find any official announcements but articles in the Daily Mail and The Grocer around December 2015 signal its demise – although the word used is ‘pause’.
The Responsibility Deal (RD) was Andrew Lansleys attempt to establish a public-private partnership between industry, government, public bodies and voluntary organisations in England. Organisations involved made voluntary ‘pledges’ on various areas, including alcohol, which are designed to improve public health and hence avoid trying to drive health improvement through regulation. Initially it was aimed at traditional targets – principally the alcohol and food industries but it developed to pick up on other areas notably mental health and health in the workplace.
I have documented some of its struggles in earlier blogs:
- Who cares about the Department off Health Responsibility Deal (2012) – this looked at its impact
- A lack of Interest – Mental Health and Responsibility Deal (2013) this explored the lack of traction of the Mental Health element of the Responsibility Deal
Its not our fault guv’
Evidence that the deal is dead is scattered around the web – this includes
- the home page of the Responsibility Deal which now has a very definite start and finish date and a statement that says that “this content was published under the 2012 to 2015 Coalition Government.” In other words its not our fault guv’.
- no mention of the public health Responsibility Deal in the latest government public health strategy produced by its agency Public Health England although the 2013/4 strategy did commit to work on the Mental Health in the Workplace Pledge – clearly not very successfully if you look at the link to on the next bullet point on registrations.
- No new registrations in 2016 and a significant drop off in 2015.
Of course the Government has to say that it was a tremendous success – just look at the evidence based (not!) statement below by Parliamentary Under Secretary of State for Public Health Jane Ellison MP this was given as part of her Responsibility Deal Presentation in March 2015.
 Who cares that it is gone?
Who cares that it is gone?
I would imagine that some of the 776 organisations who have signed up to the pledges might be a tad upset that the Government has walked away from this.
Similarly some special interest groups might also be a bit irritated at the time lost by this diversion from real policy change and activity. In my view this applies particularly to mental health in the workplace – where there is precious little activity taking place anyway.
What can be learnt
We do need to learn from this. Most importantly – and I realise this will fall on deaf ears – the Government needs to learn from this process and share this learning. Here are some thoughts:
- First – there has got to be a realistic view about when regulation is required. The main reasons for key interest groups in the public health world resigning or refusing to engage was because they were concerned that the Responsibility Deal was an inappropriate mechanism for influencing the behaviour of powerful lobby groups in the food and alcohol industries. In a number of cases (smoking, sugar) it turned out that legislation was the only mechanism that would work.
- Second I do think that voluntary processes that seek to validate the good and motivate the inadequate are a useful driver for change. Local Authorities in particular use this as way to drive improvement. However, the way the RD was set up – its crude infrastructure, vague pledges, cumbersome website, poor communications and failure to share learning meant that it was impossible to understand how meaningful a pledge was, how much traction it had in a sector and whether it was being adhered to or not. It was far too much about spin as Jane Ellison’s presentation shows.
- Finally, it is worth listening a bit more to the professional bodies. If they say that they cannot be involved because they have don’t have confidence in the model – they are probably worth listening to!
At the end of the day the level of its impact can best be measured by the deathly silence from all the organisations who signed up – that is the sufficient indication of its irrelevance.
What do you think?
Where are health Inequalities, Communities and the Voluntary Sector in the NHS England General Practice Forward View?

The General Practice Forward View is an important document, it sets out how NHS England proposes to support the development of general practice through to 2020/21. It is therefore important for all of those working in primary care and communities to understand the opportunities it presents and how it to access them.
Health Inequalities and Communities

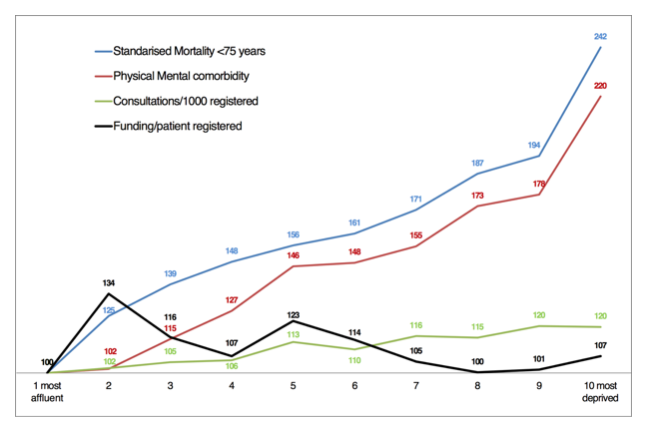
As the graph above shows it was disappointing to see that with the exception of social prescribing there appears to be little recognition given to the context within which General Practice works. So, there is little mention of inequalities and of deprivation and indeed of the voluntary sector.
This is concerning. In Sheffield we have started an exciting piece of work with practices who serve the poorest parts of the city. We recently invited Professor Graham Watt down from the Glasgow Deep End Group. Their work as is shown by the graph below (Scottish data) shows that practices serving the poorest communities are likely to receive less funding yet face much greater demands than practices serving wealthier areas.
Nonetheless the GP Forward View does present opportunities – not least because there are a range of commitments including one to revisit the GP funding formula to better reflect deprivation and rurality as well as a promise of more funding (£2.4bn more by 2020/1).
There are a number of levers for us to use – they include influencing the development of the Sustainability and Transformation Plans which will include £508m over the next five years to strengthen practice resilience (£56m), grow the medical and non medical workforce (£206m) and support practice redesign (£246m) and a development programme for practices (£30m). Similarly it will be important to ensure that CCG commissioning strategies for primary care include clear actions with regard to health inequalities and the role of the voluntary and community sector.
Here are three suggested actions.
- Data – any local authority/CCG area needs to be able to describe the particular challenge faced by practices serving the most deprived populations. The Glasgow Deep End Group focusses on the practices working in the 100 most deprived populations in Scotland. We need a similar hard edged focus. It is surprising difficult to re-create the graph above in a CCG area – but we need data on funding, health inequality and activity if we are to produce a robust evidence base that underpins actions.
- Service Models – It is the case that many GPs have developed hopeful productive working relationships with voluntary and community sector organisations. The current buzz word is Social Prescribing – but many of these relationships predate this. There is often a strong link to a neighbourhood organisation – or community anchor, many of these are members of Locality. This is important because service models and relationships will vary depending on the community. In Sheffield the recent neighbourhood based approach – People Keeping Well – based on populations of roughly 30,000 begins to recognise this level of organisation. Again, the CCG is currently undertaking a piece of work to capture different service models developed by 4 of these GP/Community Anchor partnerships. These service models should help us develop a more systematic approach to promoting ways of working that foster local partnerships with communities.
- Alliances – I know that this appears obvious. But in this case it is crucial to get General Practice staff, Active Citizens, VCS organisations and other allied services such as Pharmacy and Optometry to come together to design local service models. This is not just about consultations. This has to be an ongoing process of shared enquiry and requires different skills to the ones that NHS Commissioners have traditionally relied on. Again, we can learn from the Deep End model here who use a process of ongoing dialogue which continually spins off briefing papers and reviews. These have the potential to influence local strategies. The methodology is a bit similar to the Rapid Review approach that I referenced in an earlier blog.
What do you think?

){kind=link}