
I have recently finished (in partnership with Voluntary Action Sheffield, Involve Yorkshire and Humber, the Manor and Castle Development Trust and the Yorkshire and Humber PHO) a rapid review of Food Banks in Sheffield, which is available here – Sheffield Food Bank Rapid Review 2013. One of the issues that emerged from this work was that most food banks will only accept referrals from 3rd party agencies.
As Simon Mould – the founder of the Trussell Trust states in an article in the Guardian.
“The trust drew up strict rules to ensure it did not get dragged into doing the state’s job. It would only give out food parcels to clients who come with a voucher given to them by accredited local welfare professionals – teachers, GPs or social workers.”
On its website the Trussell Trust notes that:
“Care professionals such as doctors, health visitors, social workers, CAB and police identify people in crisis and issue them with a foodbank voucher. Foodbanks partner with a wide range of care professionals who are best placed to assess need and make sure that it is genuine.”
In our interviews it was clear that receiving referrals from 3rd party agencies takes pressure off volunteers who do not feel comfortable being placed into an assessment role – making judgements about who should or not receive support.
In Sheffield the range of referring agencies is quite broad – it includes:
Statutory Sector
- Health Centres
- Homeless and Travellers Team
- Mental Health Support Team
- GPs
- Social Services
- Multi-Agency Support Teams
- Hospitals
Voluntary Sector
- Age UK
- Homeless Charities
- NSPCC
- Asylum Seekers Organisations
- Churches
- Development Trusts
- Advice Centres
Not all food banks take referrals from all of the above. You will note that food banks are very cautious about taking referrals from any agencies funded by DWP.
I think that receiving referrals serves two other important purposes.
First – it keeps the people who receive support from food banks ‘in the world’. By this I mean that if people were able to just go directly to food banks it would be even easier for statutory agencies in particular to just leave the challenge of responding to their needs to the Food Bank sector itself. It would increase the ghettoisation and invisibility of this group of often vulnerable people.
This means that every time that a doctor or welfare rights worker makes a referral they too are reminded not just of the existence of the food bank but of the person they are referring.
Second, the food bank referral vouchers also provide an opportunity for food banks to analyse which agencies are referring most and if necessary either challenge this with the agency concerned or raise the social policy reasons for this. For example there was some real concern that some social workers were using food bank referrals as an alternative to spending crisis funding.
The Trussell Trust does use voucher information to pull together a picture about what is going on – it shares some of this information nationally. However not all food banks are members of the Trussell Trust and we found that not all food banks in Sheffield routinely collect data and fewer analyse it. I suspect that this is true across the country.
It is clear that for many volunteers their primary motivation (and rightly so) is in providing succour to their clients. Many are not directly interested in providing data to local systems and organisations. Indeed some are wary about doing it – being concerned about aligning themselves too closely with statutory agencies.
Important Local Data
Referrals are local, while national information is tremendously helpful in drawing this issue to the attention of government it is just as important that local agencies and politicians also get and use this information about their citizens and services. These small organisations are an important bellwether for keeping in touch with often vulnerable and easily ignored people.
Foodbank referral vouchers have the potential to be an important tool to understand what is actually happening on the ground. As our local report highlights one of the issues that local commissioners and Joint Strategic Needs Assessment leads should consider is how they can support food banks in gathering intelligence and analysing it.
What do you think?
A lack of interest? Mental Health and the Department of Health Responsibility Deal

The Department of Health Responsibility Deal has been in the news recently as it has claimed credit for reaching agreement with the food industry to remove one and a half olympic swimming pools worth of fat from our diet each year. Now I don’t know whether this is a big figure or not – because I don’t know how many olympic swimming pools of fat we eat each year. Nonetheless this coup allows the Department of Heath to say:
“The Responsibility Deal brings government and industry together to tackle public health issues and improve the health of the nation.”
Lets look at a less high profile area – but arguably one where the potential for impact on peoples lives is far greater – the Responsibility Deal “Mental Health and Wellbeing Pledge”
This pledge aims to “ensure that employers are committed to creating an organisational culture where staff felt valued, respected and able to flourish. The new pledge includes promoting wellbeing and resilience and challenging stigma and discrimination.”
This is a pledge that is not just about supporting people with mental health problems stay in work but is also about creating an organisational culture thats supports good mental health for all.
While the food industry example might appear to be ambitious with DH claiming that over half of the food manufacturing and retail industry have signed up, the mental health pledge actually needs to be even more ambitious this needs to affect all employers.
So it is slightly surprising that so far only 60 organisations have signed up! There is clearly a long way to go. The organisations who have signed up are a mixture of very big private sector companies (for example SERCO) and very small local businesses.
They are also a surprising mixture of statutory, private, and voluntary sectors. The 60 signatories break down as follows: 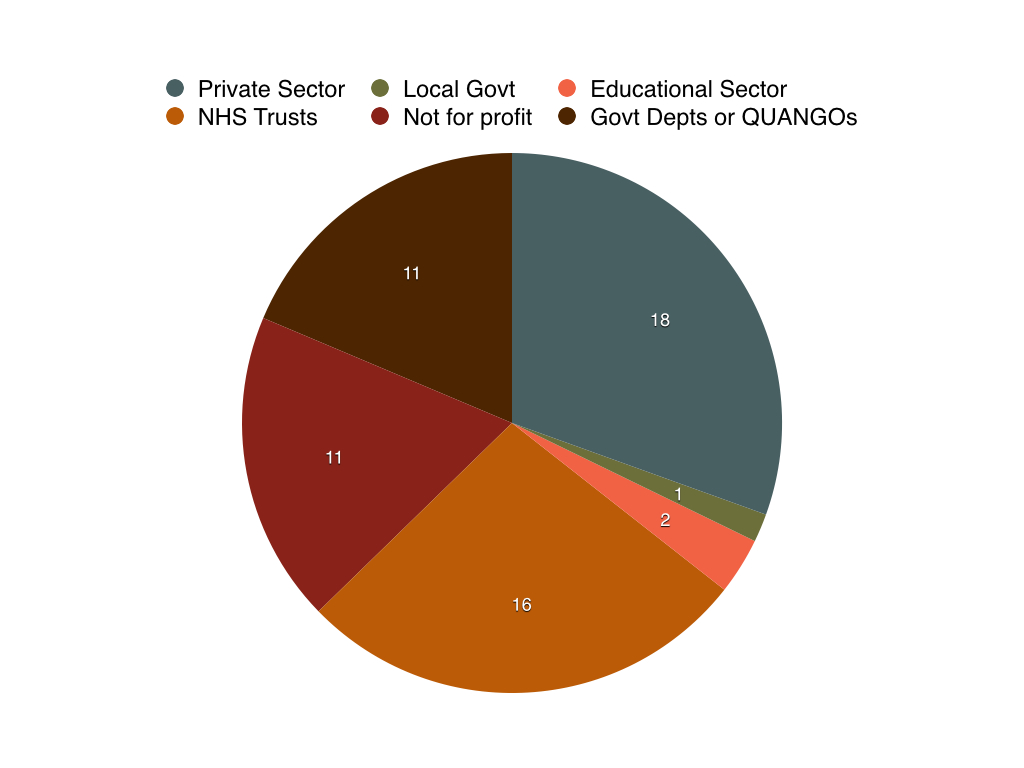 We can see that the private sector makes up approximately one third of signatories, with Government Departments and NHS Trusts making up slightly more than this and the Voluntary and Community Sector comprising just under a third with the remainder being taken up by 1 local authority and 2 educational institutions.
We can see that the private sector makes up approximately one third of signatories, with Government Departments and NHS Trusts making up slightly more than this and the Voluntary and Community Sector comprising just under a third with the remainder being taken up by 1 local authority and 2 educational institutions.
I have created a full list of signatories by sector which is here – Mental Health Responsibility Deal Membership by Sector
This is not system change!
Unfortunately the situation is worse than this. Of the 60 who have signed up to the pledge more than 20 have not published their delivery plan on the website. That means that over one third have not actually committed publicly to any action at all!
So as the following web links show organisations who have not submitted delivery plans (if they had been submitted they would be highlighted in blue as a live link) include:
- Norfolk and Suffolk NHS Foundation Trust
- Guys and St Thomas NHS Foundation Trust
- The Big Life Group
- The Royal College of Opthalmologists
- Public Health England
- Department for Education
- and so on…..
Never mind the width feel the quality!
Things get worse – there is a real variation in the quality of the actions that the remainder have committed to. I am not an expert in this field but it seems to me that there is a clear distinction between standard good HR practice – having systems in place to support individuals with mental health problems and transformational organisational culture that takes employee wellbeing – in particular their mental health – seriously.
A quick scan through the delivery plans of the remaining two thirds who have shared them shows on my count that just over 30 have in place some sort of HR policy that supports people with Mental Health problems and just over 20 have a wider ambition for culture change within the organisation and plans to address this.
I have created a full list of delivery plans by organisation which is available here – Responsibility Deal – Mental Health Delivery Plans from this it seems that only one third of the organisations who have signed up to this pledge have any plans to try to meet it!
What does this mean?
Having read through all of this stuff the first thing to say is that there are some organisations who clearly take this issue really seriously. So, purely on the basis of what they have committed organisations that I take my hat off to include:
- Adnams the Brewers
- BT
- Iceland
- Rossendales Ltd
- SERCO
- Government departments including Communities and Local Government and Department for Work and Pensions.
I have no idea what if feels like to work in these organisations – but their plans and intent seem good. However, I have to say that I would be a bit disappointed if I was in the list above and found that that organisations where who appear to be doing little are able to appear as co-signatories. That does rather devalue the commitment given by responsible organisations.
It is important to note that aside from SERCO other big outsourcing companies such as ATOS and A4E have not signed up to this pledge at all. It might be reasonable to expect government contracts to be conditional on employers supporting a pledge such as this?
Transparency
I touched on this issue in a blog a year ago. Presumably one of the main reasons for publishing this information on the website is to motivate and encourage organisations to join. I have tried to demonstrate in this post that the way information is presented on the website means that it is very hard to get a clear view about what the real picture is with regard to:
- Which sectors are engaged
- Whether organisations are large or small
- The quality of their pledge
- and so on
I suspect that if I were to look at other pledges I would find the same deficits I have identified here, which does make me rather sceptical of the government’s trans-fat claims that I mentioned at the start of the blog. The way in which the information is presented, the poverty of analysis, the lack of quality control speaks not of responsibility but of lack of support and disinterest….by the Department of Health.
What do you think?
Do Local Authorities need a Director of Public Health?

As local authorities start to get to grips with their new public health responsibilities there is the inevitable jostling for position and power in terms of where the public health teams sit.
In the non-statutory Public Health England guidance (produced jointly with the Local Government Assocation and the Faculty of Public Health) on appointment of directors of public health by local authorities there is a clear position that the Director of Public should have “accountability for acting as the lead officer in a local authority for heath” and “to enable them to carry out their role effectively there must be direct accountability between the DPH and and the local authority chief executive”. In most cases this is taken to mean that the Director of Public Health should have equal standing at the Executive Team as others such as the Director of Adult Social Care.
Some local authorities have not fallen obediently into line on this and have instead had the DPH reporting to the Director of Adult Services or even, as in Lancashire have had a none Faculty member take on the DPH role.
I think that some of the reasons why there has not been a consistent adherence to this model have been:
- Directors of Public Health being outmanouvered by other senior officers who understand the local authority environment better and have more credibility.
- A failure to demonstrate that DsPH responsibility equates to the statutory responsibilities and larger budgets of a Director of Adult Services or equivalent.
- Local Authorities already feeling confident that they have a good grip on strategies to address the health of the public with their existing top team – for example Lewisham where the head of Community Services manages the DPH.
While I have not been able to check this thoroughly there are roughly 26 Directors of Adult Social Care who include ‘health’ in there title (ADASS Members with Health in Job Title). This equates to approximately 5% of all Directors of Adult Social Care. Of these it is clear that some see themselves as the most senior champion for health in their local authority and in some cases probably manage the DPH – for example Derby.
Despite this I think that in the majority of cases most Directors of Public Health are in the top team reporting directly to the Chief Executive. But, as Mary Black in her good blog on the Faculty of Public Health website notes
“Those of us who are (on the top managment team) will need to demonstrate pretty fast that we deserve those seats and in some places we may well struggle to keep them. We have another 18 months, perhaps less, to prove our value.”
What is also interesting is that in addition to people like Mary who have a realistic and positive story to tell there are others who appear to have gone even further. So in my list of 26 Directors of Adult Social Care three of them are actually Directors of Public Health. Maggie Rae in Wiltshire, Richard Harling in Worcestershire and Paul Edmondson-Jones in York – whose job title is Deputy Chief Executive and Director of Public Health and Adult Social Services!
When we look at the structure chart for Wiltshire it is quite clear that Maggie is responsible for leading on Adult Social Care.
So, what we have here is a bit of a two way street. Some local authorities have clearly been impressed by the skills and experience of their Director of Public Heath and considered that these mean that they should also take on the Adult Social Care portfolio. While others have been more impressed by what the Adult Social Care profession has to offer and gone down that route.
Now, I don’t subscribe to the Association of Directors of Adult Social Care ebulletin so I have no idea if Sandie Keene their President is outraged by this colonisation of her territory.
I do subscribe to the Faculty of Public Health ebulletin and I know that John Ashton the Faculty President is not sanguine about Adult Social Care leading on Public Health.
“It is ludicrous to have the situation, as there has been in Lancashire, where a social worker is appointed Executive Director of Social Services and Public Health. We must be clear where we stand on issues such as this and draw lines in the sand. Social workers are most welcome to come to us and train as public health specialists and consultants”
FPH Bulletin – Issue 102 – August 2013
This is of course a serious debate
- Local Authorities are under the cosh from central government – they simply cannot afford large Executive Teams – its is inevitable that they will seek to rationalise and merge senior management roles.
- Local Authorities will need to focus on what difference they can actually make to the health and wellbeing of their citizens – in particular those who are the most vulnerable.
- The priorities they decide to focus on will play a significant part in determining what sort of person they feel should lead this at the most senior officer level.
There is therefore an urgent need to consider how best to ensure that local authorities and their partners are offered appropriately trained professionals who they can afford to pay.
If localism means anything then we need as a profession to consider how to support confident local authorities like Lancashire, Wiltshire and York to have the freedom to choose the best person for the job and not to be constrained by closed shops.
It is clear that for some local authorities the key issue is competence not the ‘FPH badge’ I suspect that this trend will continue. We therefore need to be developing a refreshed idea of what public health in local authorities might look like. Part of this must be through developing a shared dialogue with the other partner professions who have been working in local government and in many cases making it work well for the 40 or so years that Public Health has been in exile in the NHS.
What do you think?
Leadership, Passion and Patient and Public Involvement

Now that the NHS England Guidance on Transforming Participation in Health and Care is out I thought I would return to one of the areas that I think needs exploring further.
First, lets be clear – the guidance is helpful, it is comprehensive and includes lots of examples of good practice with easy access to back up material. However it is technical guidance – it is concerned with how to do it – it does not directly address the leadership role of the CCG in partnership with the local authority for setting the tone and ambition for Patient and Public Involvement in a place. Not addressing this risks PPI remaining something that can be turned off and on by commissioners because it is not culturally embedded in the local system.
Local Authorities and CCGS must work in partnership to lead on promoting good practice on participation locally and on making it happen. This is a leadership issue.
Leading Patient and Public Involvement
As I said in an earlier blog I think that there are a small number of organisations who have leadership role for patient and public involvement at a local authority level. There are not many of them – they are:
- The Local Authority
- The Clinical Commissioning Group
Good Practice in provider organisations
Then there are those organisations that have a major responsibility in ensuring that their practice with regard to patient and public involvement is as best as it can be. Key ones include:
- NHS Provider Trusts
- Social Care Providers
- Voluntary and Community Sector Care Service Providers
- Private Sector Providers
- Other Providers who services improve wellbeing like Housing, Education etc.
While they have responsibility within their organisations but no formal responsibility for leading good practice at place level. However, their scale and the fact they they provide the services means that this is the arena where the bulk of PPI happens. I think this is a challenge for commissioners.
Delivery of Voice and Advocacy
The third group of organisations are those funded to support the development of Patient and Public Engagement and delivery of voice – many of these are in the community and voluntary sector these include:
- Advocacy Organisations including Healthwatch
- Infrastructure organisations such as Councils of Voluntary Service
- Healthy Living Centres and Locality Members – who may provide community development services.
Wider Organisations
Finally, there are organisations who have an important contribution to make to fostering citizenship and engagement – many of these are in the education and learning sector – schools, further education, the Workers Education Association and Universities.
Crucially this is not just an agenda for the health and care system – as I have said in earlier blogs it is essential that health contributes to citizen engagement more generally. I know this is obvious – but health will struggle to move services from hospital to community or address the social determinants of health unless it recognises that it has a key role in contributing to a wider citizen engagement agenda.
I think that their is a real danger that unless CCGS are clear about their leadership role at local authority level with regard to PPI then their focus will be predominantly on how they commission services rather than also considering how people are enabled to engage, participate and contribute to improving health and wellbeing in an area.
Here is a diagram that tries to encompass some of this:
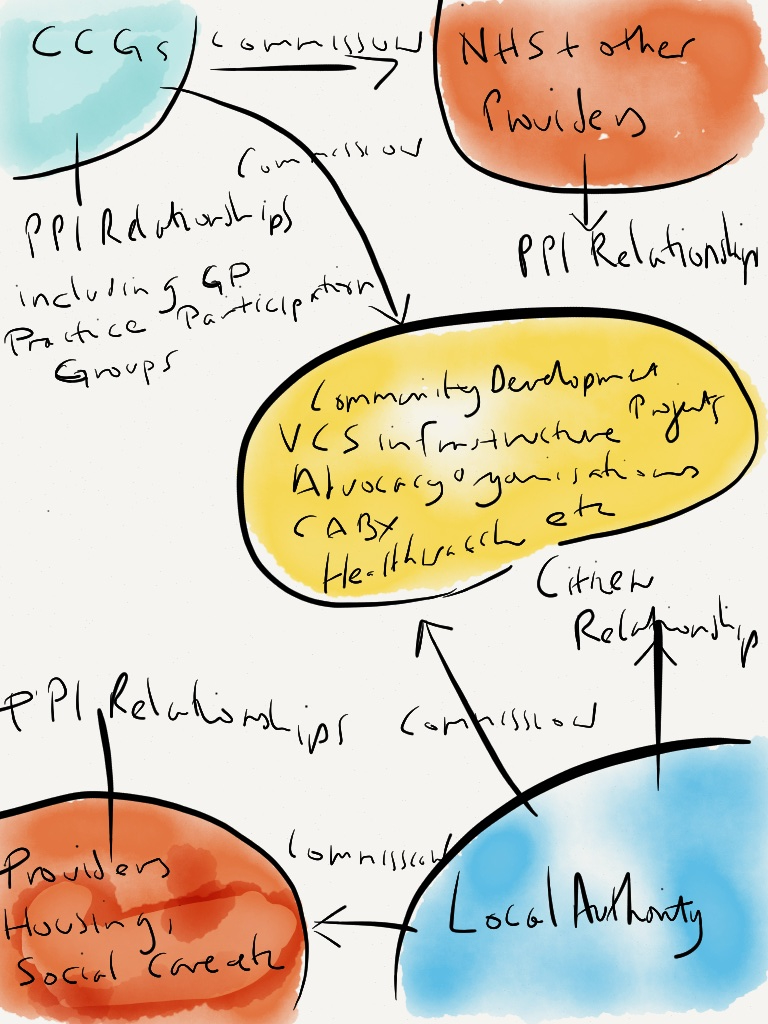
So here are some actions that I think fall from this.
- First, CCGs need to empower those with a responsibility for PPI in their organisations. This must require some sort of structural mechanism – a strategic PPI committee which reports to the board. Membership should include Non-Exec PPI leads, relevant directors, Healthwatch it should also have strong links with big NHS provider organisation PPI leads, and link to the local authority and VCS.
- Second, CCGs should work with local authorities through the Health and Wellbeing Board to develop a local authority level Community Engagement strategy this needs to reach out to a wider agenda that includes the development of volunteering, community development, etc – part of this must include a joint commissioning plan that sets out how key infrastructure organisations are supported.
- Third, this is a developing area – no one has the right answer. CCGs need to be seen as one of the key organisations that are interested in co-producing solutions. So, CCGs should use their position to foster an ongoing programme of debate and dialogue sharing ideas, good practice etc to drive innovation and strengthen energy. This needs to be a place where individuals, the community and voluntary sector, health and wellbeing agencies and the academic sector come together.
Patient and Public Involvement is not a dry technical process – its an emotional one! People get involved because they are passionate about the health system, concerned about their own health and want to contribute to make things better. We need to work in a way that harnesses this energy and celebrates the challenge!
What do you think?
Child Health and inequality the role of Citizens Advice Bureau, Nurses and Health Visitors
This is a story about two conversations.
The first was a passing chat with a Danny Dorling a few years ago – lets be clear I am not claiming that this happens very often! We were talking about how children from low income families are more likely to die at birth or in infancy than those born in the richest areas and are are more likely to suffer chronic illness during childhood (see Child Poverty Action Group for more evidence on this)
His theory was that precisely at what should be a joyous and celebratory time – the birth of a baby – families on low incomes experience increased stress and pressure which should be preventable. The scenario he set out was a bit like this.
A family is just about getting by financially and then a new child arrives – not only do they have all the additional work and expense associated with a new baby but their income might be reduced if one of them has stopped or reduced working hours, they may experience greater employment insecurity, and they may already have other pressures poor housing, indebtedness etc.
Of course they will be entitled to some financial support from the state such as maternity grants, Child Benefit, Child Tax Credits etc however, this might take a while to play in.
So while there is support there – the combination of a new child, any existing financial stress, the complexity of the benefits system and its responsiveness can mean that the health and wellbeing of young children in poor families is under greater and unecessary risk for a period of time.
This view is supported by Sir Michael Marmot:
“First time pregnant mothers dependent on Income Support find their level of income particularly challenging. …pregnant women in receipt of benefits remain vulnerable, especially if they are under 25 and only receive lower age benefit rates for themselves, making it difficult to maintain a healthy standard of living” (Quote from Strategic Review of Health Inequalities Post 2010 Page 117)
Of course this is also in an atmosphere where the government is increasingly describing people on low income as underserving which may put some people off claiming what they are entitled to.
Steps to a solution
The second conversation I had was last week at the Citizens Advice annual conference. This was with the Jeremy Vanes who is the Chief Executive of Wolverhampton Citizens Advice Bureau. Jeremy told me about an initiative that they are running – funded by the Wolverhampton City Council Public Health Department.
This is basically a maternity advice hotline that aims to address precisely the issue that Danny described.
The project aims to give top priority to this group – supporting them get right to the front of the queue. The key agents are health professionals who are encouraged to use a simple pathway to support the parent – usually mother access advice and support.
Jeremy told me that the original champions were midwives – but they have now broadened this to a wider group of professionals who are more community based – School Nurses and Health Visitors and referrals to the hotline have gone up.

It is still early days so as far as I am aware the programme has not been evaluated. However, the programme feels really strong joining up a social determinants of health intervention with the delivery of NHS care. It is targeted at the most vulnerable and it comes in early and therefore has the opportunity to be genuinely preventative.
As the government gets ready to announce the 17 successful Integrated Care Pioneers shouldn’t we expect initiatives like this to be at the heart of this work?
Update
Since I published this piece Jackie Erdman has got in touch and drawn my attention to this really useful evaluation of a piece of work in Scotland. She says “We have developed an intervention in Glasgow and Clyde aimed at women and children and taking a gendered approach to child poverty. Over the last 2.5 years this has generated over £4 million in benefits and debt reduction for children and families, as well as other benefits such as help in kind.” The initial evaluation is available here: Healthier Wealthier Children Project. She says that a further evaluation is due shortly.
Do you know of any other examples of this sort of intervention?
What do you think?
Transforming Participation in Health and Care – what should Clinical Commissioning Groups do?
 NHS England are currently coming to the end of a consultation on a guide titled Transforming Participation in Health and Care. Its always risky to have titles like this – because stakeholders then look to them with raised expectations. Sometimes I think it might be better to go for titles such as “Improving things little by little – participation in health care” or “Steady as she goes – some ideas about improving things a bit in participation in health care”!
NHS England are currently coming to the end of a consultation on a guide titled Transforming Participation in Health and Care. Its always risky to have titles like this – because stakeholders then look to them with raised expectations. Sometimes I think it might be better to go for titles such as “Improving things little by little – participation in health care” or “Steady as she goes – some ideas about improving things a bit in participation in health care”!
I am not going to comment on the document directly. Here instead are five areas that I thought about when I read the document – some of these are mentioned in the draft guidance others are not or are not mentioned strongly enough.
Role of Clinical Commissioning Groups.
The old NHS paradigm sometimes felt like it was based purely on how each commissioning or service improvement process involves the public. While this is important if we are to genuinely transform participation in health care CCGs also need to provide place leadership in partnership with local authorities to shape how the local health and wellbeing system involves the public.
Unlike provider organisations CCGs have this system level responsibility.
So, this cannot just be about involving the public in individual commissioning processes that CCGs manage. It has to be about CCGs sharing responsibility for how an area (local authority level) provides ways for citizens to participate in the local health and wellbeing system.
Clinical Commissioning Groups therefore need to work with providers to ensure that they have powerful systematic actions for ongoing public involvement. In particular as a member of Health and Wellbeing Boards CCGs need to ensure that the participation of the public occurs across service AND organisational silos.
CCGs must also promote (with local authorities) a shared approach to driving forward good practice and building local capability. This should include explicit strategies to:
- Build local capability and capacity at a system level – to enable citizens (particularly from disadvantaged communities) to build on their interest in their health and wellbeing and that of their families and communities so that they can confidently get involved.
- bring joint investment to key local infrastructure organisations
- ensure explicit approaches to working across services and organisations to share practice and information and report on these to the health and wellbeing board.
- Championing dialogue and challenge across provider organisations
Effective Models of Participation by the Public in Commissioning.
Many of the models of Commissioning that are promoted by the NHS tend to be neat and tidy – for example the old World Class Commissioning Model – this graphic is taken from the Patient and Public Engagement Toolkit – South Central:

These flow charts reflect how commissioners imagine the world to be not how it actually works – they are led by how finances are organised; financial year reporting requirements; 3 year funding programmes; target delivery requirements and election cycles. They do not reflect how we live our lives as citizens and what we need in order to engage and influence.
We need models that start from how the public experience the world not how the system feels the world should be. For example I do not manage my personal relationships on the basis of some conceptual model of needs assessment, analysis, commissioning, review and recommissioning. Of course those of you who know me might argue that I would benefit from this!
So, CCGs will need to recognise that developing relationships with people in order to increase accountability and strengthen co-production actually requires approaches that foster stability, consistency and the long term. They need to provide flexible, long term points of entry built on trusted relationships – such as those developed by neighbourhood organisations like development trusts and healthy living centres.
So I think that a public centred model for participation might look a bit like this:

Active relationships with an empowered public
Powerful relationships with the public require commissioners to take a balanced approach to investing in support – this means taking a shared responsibility with local government in particular for the relationships that people have with sectors and institutions. It is crucial therefore to share responsibility for commissioning key local institutions such as Adult Education, Voluntary Sector Infrastructure Organisations – such as those that support volunteering and generic and specialist community development organisations – particularly those that operate at a neighbourhood level.
It also means recognising that it is important to foster mechanisms that promote dialogue and challenge. I am actually not convinced that we should have a core target that 80% of stakeholders should be feeling satisfied with regard to how CCGs have involved people. Dissatisfaction and disagreement are powerful drivers for positive change – promoting targets that call for high degrees of satisfaction feels really dangerous to me – not least because as Ibsen tells us “the majority is always wrong”!
Knowing what is going on
Clinical Commissioning Groups must work through Health and Wellbeing Boards to establish agreed ways of testing whether the level of public participation and involvement is adequate. I think that Health and Wellbeing Boards with active support of the CCGs should be commissioning intelligence reviews that capture the level and type of engagement that is happening within the health system so that providers and commissioners can be held to account for the degree involvement and participation.
Lets face it we could all benefit from a continuing evidence based dialogue to help us build on good practice and tackle areas of weakness. Frankly if Francis tells us anything at all it should be that we need to establish mechanisms locally that stop us deluding ourselves that we are ‘good’ at participation.
Volunteers
I do think that any guidance on participation has to recognise the key role of volunteers. These are people who are actively involved in co-production. Either through delivering services or helping to develop or manage them. I think that there is a strong relationship between the number and quality of volunteers and the effectiveness of work to increase participation.
What do you think?

I have now read this document three times – and am still unsure what to make of it.
The Call to Action – is spearheaded by NHS England with signatures from a number of NHS bodies and the Local Government Association. It sets out a challenge – how to maintain a National Health Service that is free at the point of use and able to effectively respond to 21st Century health and policy challenges.
With the exception of Cllr Zoe Patrick who is the Local Government Association (LGA) Health and Wellbeing lead all the signatories are the senior officers of the signatory organisations. However, I can find no evidence that this has been discussed at the LGA Community Welleing Board (which Cllr Patrick chairs) in May or July of this year.
There are no signatories from provider organisations such as the NHS Confederation (with the exception of local government) or from interest groups such as the NHS Alliance and of course there is no ministerial name here.
- While the call to action is clearly a commendable attempt to generate some debate about our approach to health services in this country and influence their future shape it is also of its time.
- It is also a statement of mandate and independence – creating clear space between government and the system management organisations it has created. This is the first time I can remember that national NHS bodies have sought to create a dialogue which seeks to inform and influence government policy.
- It is an attempt to connect more with the public – it fits with NHS Englands ideas around the NHS as a ‘social movement’ which I touched on in an earlier blog.
- Finally – although there are no timetables in this document I would guess this is in part an attempt to influence the manifestos of parties prior to the next election.
Where is mental health? As is far too common in official NHS and Government material – there is little about mental health in the document a passing reference to “we need to do far more to help those with a mental illness” will not do.
The Analysis states that….
- There needs to be a greater focus on prevention
- The quality of life of people with long term conditions needs to be enhanced
- There is more demand on A&E and urgent admissions – which is concerning
- Patient experience and safety while good need to be improved
- Health Inequalities – there remain persistent and unfair differences in health, illness and life expectancy
It identifies a number of challenges….
- Ageing Society – according to a report by McKinsey the largest proportion of health and care spend is concentrated on providing health and social care to people over 75. This proportion will increase both with regard to physical health and mental health – in particular dementia.
- Long Term Conditions – people with long term conditions (many of whom are elderly) place a significant demand on the healthcare system.
- Impact of non-communicable diseases in the future – predictions are that by 2035 46% of men and 40% of women will be obese.
- Health services are getting more expensive. The huge investment in technology led medical improvement has led to higher expectations from the public and an increase in expensive interventions.
- Limited financial resources – A recognition that the NHS budget will at best not grow and that government cuts in social care increasingly affect the NHS.
The document identifies some possible areas for debate such as….
Prevention – Should we invest much more in in prevention? I think the question here is still framed too much around health and care – and needs to be broadened to include the social determinants of health.
The Public – How do we give patients (the public?) greater control over their own health?
Targeting – Services need to be more tailored. Although it does not say this – this is of particular relevance to easily ignored communities and people.
Economic Growth – “the NHS is the single largest customer for UK health and life science industries”. There is a bit of an irony here – NHS and Government funding into such institutions as the NIHR are overwhelming focussed on clinical and technological interventions – yet the document calls for greater investment in prevention and personal control. Its no good making the economic case for change and calling for continued investment in expensive high tech interventions.
Call for debate
This is the bit where I start to struggle – the proposition is that NHSE will lead a national debate on priorities and that this (“biggest debate ever”) will feed into Clinical Commissioning Groups in 2014/15 and 2015/6! What happened to localism?
Like many other people I am involved as health and wellbeing activist where I live. Yet this call to action does not engage with me – it feels like a distraction to local work – I struggle to see how this helps us develop a stronger local voice.
This feels short term, exhausting and top down.
We need more than what is proposed. Here are two things that I think would help:
- NHSE and all its partner organisations need to support an assertive and practical programme of long term investment in building local understanding about health and wellbeing and how to influence and change it. As it stands the “call to action” feels like yet another short term consultation. We need a sustained programme of significant investment in building citizen led confidence and capability at a local level in what works with regard to health and wellbeing. This means investing in local organisations – local authorities, Clinical Commissioning Groups, local Healthwatch and voluntary sector organisations, adult education institutions and others to build ongoing local democratic debate and engagement in health and wellbeing.
- Local government has to lead this through Health and Wellbeing Boards. This means that national NHS organisations need to embark on a humble dialogue with local authorities to co-produce a joint approach to this process. I am unconvinced that the current document is a product of such a collaboration.
It means letting go
What do you think?
Volunteers and Local Healthwatch
One of the biggest challenges for local Healthwatch is how to best mobilise the many members of the public who want to contribute to improving local health and wellbeing systems.
who want to contribute to improving local health and wellbeing systems.
The challenge that Local Healthwatch faces is how to do this in a way that makes a system level impact. In this they are no different to LINKs and face the same pitfalls – the main one being to focus almost exclusively on recruiting their own volunteers.
I think that the LINK model put a great deal of emphasis on three types of voluntary engagement these were:
- A board of volunteers
- A team of volunteers providing services – information, office, enter and view etc
- A wider membership – who were comparatively inactive.
I do know that some local LINKs also engaged and worked with other organisations who also recruited and worked with volunteers and also with user led groups (patient and carer groups) which were run by people with a specific condition.
My impression was that for many local LINKs their energies focussed on supporting a comparatively small and dedicated group of volunteers – which took their energy away from wider system level ambition.
For Healthwatch to be powerful it has to locate itself within a wider context of volunteering at place level and its actions then stem from this understanding of context.
I have been messing around thinking about how to describe this context and have come up with this strange looking diagram – “the knickerbocker glory of volunteering ”.

The diagram suggests that there are 3 ways of considering volunteering with regard to Healthwatch which are connected and have different degrees of importance.
These are
- Healthwatch Volunteers;
- Health System ‘Voice’ Volunteers – where giving opinions or advocating is a key part of the role;
- General volunteers in the Health System who are providing services of different sorts – such as WRVS or people who provide luncheon clubs.
Running parallel to this ‘Health System’ strand are similar groups of volunteers who are also concerned with voice – such as school governers, welfare rights volunteers, trade unionists etc and a similar much wider group of volunteers involved in everything from culture through to environment. This group is of course equally important because health is not just about health and social care. The Social Determinants are equally important and these voice volunteers will be interested in a health and wellbeing too.
Here is a table showing the sort of volunteers that I am talking about (N.B. PLACE assessors are people who use a health service including current patients, their family and visitors, carers, patient advocates or NHS patient council members. PLACE stands for Patient Led Assessments of the Care Environment) Bear in mind that the volunteer roles in the table below are just examples – there are many more!
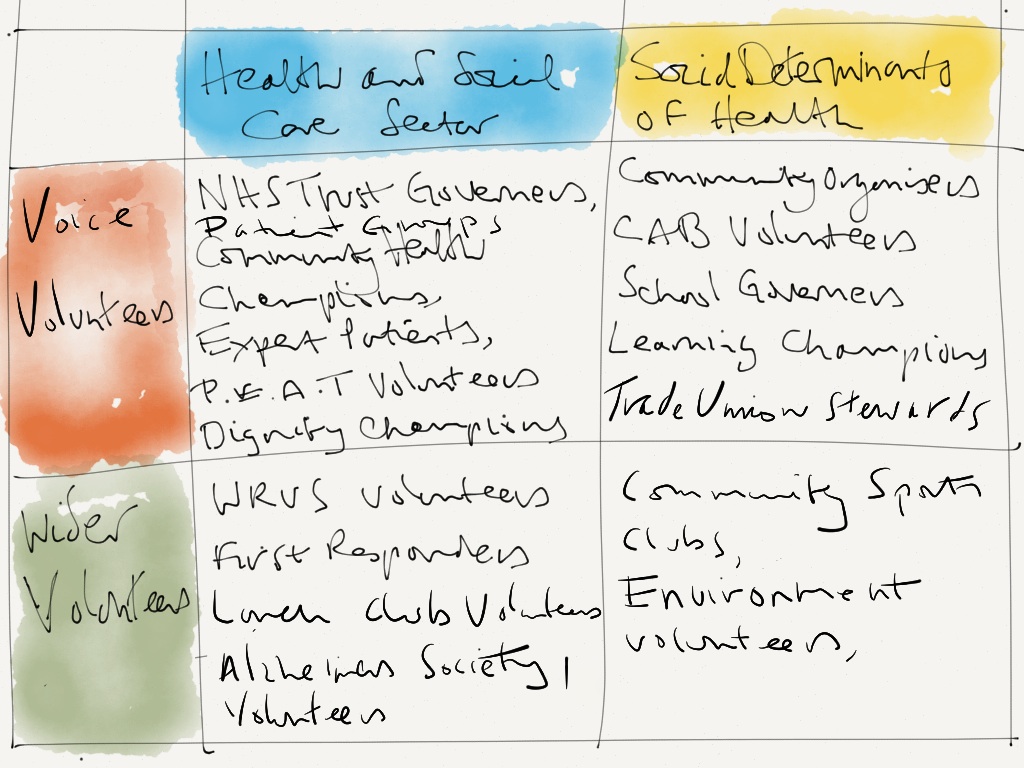
Obviously, its not possible to be connected directly with all of the volunteers described here. My argument is that a powerful Healthwatch will as a minimum have a strategic approach to being connected with all organisations who recruit, support and train ‘Voice Volunteers’ whether they are in the Health System or not.
What do you think?
Public Health England – How helpful is Longer Lives?
Its difficult being a new organisation – particularly when you are so close to your main funder that it is hard to see where the join is. This is the problem faced by Public Health England.
to see where the join is. This is the problem faced by Public Health England.
Public Health England is an Executive Agency of the Department of Health this means that while it is treated as being managerially separate from the Department it does carry out some of the executive functions of Government.
So, when Public Health England announces something we should see this as being as a Government Position.
So the announcement on Tuesday the 11th of “Shocking” local variation in early death rates across the country appears to be official recognition that health inequalities is still an issue of real concern to Government…..except that health inequalities is not mentioned at all.
What I want to focus on is how the data is presented and what the underlying message is – because this information sets the tone for government discussions with local authorities and will be the information that Directors of Public Health in particular will be taking into Health and Wellbeing Boards.
The Big Killers
Despite Government commitment to give equal weighting to mental health (see foreword of No Heath without Mental Health) the Longer Lives website ignores this and instead focusses on the old medical public heath favourites of Cancer, Heart Disease and Stroke, Lung Disease and Liver Disease. These are all presented with regard their impact on early death.
So, in this the first significant product from Public Health England for local authorities and Health and Wellbeing Boards the early messages are:
- Its early death not long term illness
- Its physical health not mental health
Blame the Poor
As well as the focus being on “the big killers” the proposed interventions are weighted heavily towards lifestyle three quarters of the interventions focus on behaviour change. In other words teaching and persuading people to accept their circumstances and improve their behaviour. The graph below shows that of the proposed interventions approximately 3/4 focus on lifestyle change. (My workings out are here – PHE Blog)

Collectively they give a very dubious message to Health and Wellbeing Boards which is:
- Prioritise telling people to live more healthily
- Don’t worry about how they feel
- Don’t worry too much about their socio economic circumstances
Comparing apples with pears
I think that the way the data is presented replicates a mistake made bythe last government which grouped those local authorities with the greatest health inequalities compared to the national average into ‘spearheads’. This meant that local authorities with a large middle class population and a large deprived population appeared to be less challenged than those with where the majority of people were deprived – even though they might have more people who were experiencing inequality.
The way the data is presented feels inaccurate because it is comparing average premature mortality at local authority level. This means that very deprived communities within local areas can be masked by more affluent ones.
What happens next
Local Authorities and Health and Wellbeing boards are working on much broader approaches to improving health and wellbeing that recognise the importance of mental health and the impact of the social determinants of health. It will be important that the governments narrow view of priorities and how to tackle them does not divert them from this agenda.
What do you think?
As the great beast that is NHS England gets up and running it is already proving challenging to keep up to speed as it churns out ideas, instructions, promises and commitments.
speed as it churns out ideas, instructions, promises and commitments.
So as small local organisations like Healthwatch have their heads down establishing mechanisms for citizen engagement NHS England enters stage left with its own ideas…….
The Civil Society Assembly.
In a paper to the February 2013 NHS England Board (or NHS Commissioning Board as it was then) Tim Kelsey proposed that it establishes a “design group to explore the creation and development of a citizen and community assembly through enabling a civil society movement that brings transparent accountability and a powerful voice for patients and the public to NHS England”.
This is to:
“build citizen voice and influence throughout the NHS commissioning system, so that citizens hold the NHS to account, driving improvements in quality and outcomes.
I agree with this part of his analysis:
“People have a passive relationship with the NHS and their activation is generally low. The paternalistic medical model of health is not conducive to equitable person-centred approaches to involving people, their families and communities”
He then goes on to say:
“Co-designing and creating an independent ‘Civil Society Assembly’ could be the means through which NHS England can directly engage with citizen voice in a publicly accountable and transparent forum.”
The paper is clear that previous attempts at patient engagement have too often attracted the ‘professional patient’ and it has too often been white, middle class, aged/retired professionals.
The paper calls for NHS England to go beyond the ‘usual suspects’ or the ‘expert patient’ reps instead going into communities whose primary issues may not be ‘health’ but other social determinants that have a major impact such as housing and employment.
It also acknowledges the need to develop a complementary approach with Healthwatch England to ensure mutual benefit.
The paper sets out the following ambitions:
- Public Accountability – an independent and critical mirror for NHS England
- Co-design, advice and reflection – a forum that stimulates ideas, tests thinking and draws experience and evidence together
- Challenge – a critical and challenging friend
- Voice – of the hardest to hear, most marginalised and most vulberable
“It will be a catalyst for a social movement that engages and stimulates new, emerging and established groups and organisations to connect”
Its helpful because………..
We never heard of any attempt of trying to build citizen voice into the old Strategic Health Authority structures and certainly not into mechanisms established by the Department of Health.
Indeed when I once offered to organise a regional meeting to bring the Chief Executive of an SHA into dialogue with local community health champions their reply was “why would I want to do that?”
So national recognition that engaging with citizens is crucial. This will help cultural change in NHS England which might then drive local engagement and help improve service quality.
Its unhelpful because………
This issue is more important than this – the proposal lacks an analysis of context for example:
What happened to localism? If NHS England wanted to be truly radical it would thoughtfully consider whether it might be better served by strengthening its relationship with local democratic structures rather than going for a quick fix national forum. For example it could:
- invest in supporting the only form of local accountable governance – local government – helping it to become stronger and more effective in bringing local accountability to the NHS.
- In partnership with local government it could invest in supporting Clinical Commissioning Groups significantly improve their practice with regard to developing local accountability and engagement.
- It could thoughtfully consider whether a better understanding of and support to existing arrangements – Health and Wellbeing Boards, Healthwatch England, Local Government, CCG arrangements and VCS contributions could be strengthened and how it could support them in developing a coherent national voice.
Actions NHSE could consider
- Get the language right. These proposals reek of hubris ‘establish a social movement!’ I thought this nonsense had died with the NHS Innovation Institute. In my experience social movements do not emerge through dictat. Although it would be fun seeing Malcolm Grant championing the social movement model on a national platform.
- It might be better to build, invest in and foster engagement with the public around institutions that are appropriate and unlikely to disappear. Tactically this certainly means local authorities and the voluntary sector and probably NHS hospitals and GPs. We can be confident that any ‘social movement’ built around NHS England will have a life of no more than 5 years before NHS England is being re-organised – I know that I am being optimistic here!
- By all means foster national good practice – but the focus should be on supporting existing local democratic structures. NHSE needs to consider how it is held to account through Health and Wellbeing Boards (of which it is a member) and needs to put intellectual and material resources into ensuring this process works well – build up from the grassroots rather than impose a national structure.
- Finally – try to stick to the values! The original paper which was presented to the NHS Commissioning Board on the 28th of February 2013 recommends that the the Assembly must be independent of the board (para 10). One month later the NHS England business plan has already given the ‘independent’ civil society forum a target! In the key deliverables section opposite para 3.131 it states that “The Civil Society Assembly demonstrates over 80% satisfied with the involvement of patients and the public in the planning and commissioning of NHS services by NHS England. This is a target for an independent forum that has not even been set up yet! I suppose NHSE are to be congratulated here because they have managed to move in the space of 1 month to the third stage of social movement development – bureaucratise!
What do you think?

{kind=link}