I am involved in 3 local Healthwatch and as they get going one of the first things to think about is the process of setting priorities.
At the moment there are two things I am thinking about.
The first is how to select the priorities of today?
I think that one of the biggest challenges is getting the balance right between the memberships views and other views of priorities. An approach that gives too much weight to building a workplan based purely on the views of its membership runs the risk of setting priorities that do not reflect some of the real underlying concerns that need to be addressed within a health and wellbeing system.
It also lets the Healthwatch organisation off the hook – allowing it to say ‘this is what our members said were concerns’ and therefore not taking sufficient responsibility for addressing important system level concerns that the membership did not raise.
I think that there are three key areas that a local Healthwatch needs to consider and it is the way in which it manages these that then help shape local Healthwatch Priorities.
These three areas are summarised in the diagram below:

The Official Line – What key public documents say
I think the first place to go are the reports produced by public organisations. I am still feeling my way here but would suggest that this should include:
- The Joint Strategic Needs Assessment and Joint Health and Wellbeing Strategy
- Quality Accounts
- Local Accounts
- Relevant CQC Reports
- What other documents would you add?
There is a limit to how many documents a small organisation can read but I think that the above list are probably the essential ones. The key issue is to consider these seperately from any official consultation process. Together these documents represent the official shared narrative of priorities and quality in a place. This is not of course the same as a true narrative!
The Unofficial Line – what the professionals say
Many managers and directors in key organisations will have a clear professional view of system level challenges and failures. A lot of them will be working hard to champion improvement and will be finding it slow or worse. Some will be keen to share their concerns informally – in the hope that some external pressure or interest will help them drive work forward. A gentle process of informal dialogue with a range of key managers will help test ideas about where to probe, investigate and test.
Voice – what the public say
This is clearly crucial. I think that one of the challenges is how to use this important democratic mandate to greatest effect. Listening to the views of the Healthwatch membership and special interest groups is not enough. This has to be about building a mandate through dialogue with these groups. I think this will mean taking a risk and presenting an analysis based on the official, unofficial and voice information and being willing to debate this and amend it with the membership – producing a set of priorities through this process.
The second issue I am concerned with is how to strengthen the democratic voice in the future?
In many cases Healthwatch has inherited quite weak processes from the outgoing LINK (I know not all!). I do think that now is the time to recognise this and it is reasonable to focus some energy in year one on working with key stakeholders to establish processes to improve public engagement processes for the future. It is in local Healthwatch’s interest to ensure that the system as a whole puts energy into raising its game with regard to public engagement as a priority in year one.
What might this look like?
In year one this might mean convening a cross sectoral group involving the PPI leads from the CCG(s), Local Authority, NHS Trusts and big care service player to consider how public voice plays in across their organisations and the local system.
For example:
What is the balance between:
- Membership
- Complaints
- Consultation – individual and collective
- Representation – from membership/patient fora/governers and none exec directors
- Co-production – from focus groups to volunteering
- Feedback – how does this happen?
What support is available for the public (patients, people using care services, carers, the public as a whole, people who experience discrimination) to engage and participate for example:
- Information provision
- Training
- Interpretation
- Community Development Support
A shared view about deficits and ambition would help lay the foundation for a system that places a greater emphasis on public involvement in priority setting in future years.
What do you think?
Who are the Citizen Champions for Health?
In a still small but growing section of the health world we are increasingly familiar with the idea of ‘community health champions’. As Altogether Better say on their website
‘Community Health champions are people who, with training and support, voluntarily bring their ability to relate to people and their own life experience to transform health and well-being in their communities. Within their families, communities and workplaces they empower and motivate people to get involved in healthy social activities, create groups to meet local needs and sign post people to relevant support and services.’
One of the things that has concerned me about ‘Health Champions’ is that we can achieve wellbeing outcomes through other forms of activism that are equally valid. These are some of the characteristics that I would use to describe what champions do:
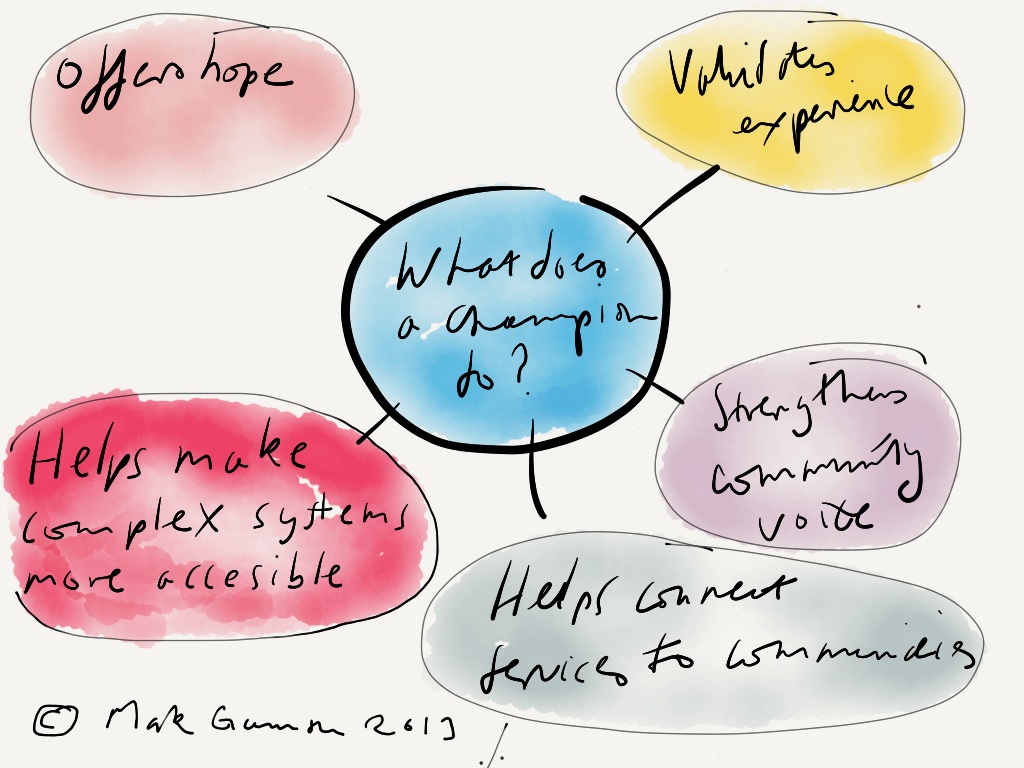
The point is that that “Champions” are not exclusive to the Health System. We would be mistaken in thinking that the only form of champion that can help us improve health and wellbeing are those who have got “health” in their title. We know that the social determinants of health have a much greater impact on our health than health and social care services. So it is in our interest to recognise, encourage and validate other sectors that are also promoting active and strong citizenship through champion models.
Here are two important examples:
Some of the key players supporting Community Learning Champions are the Workers Education Association and National Institute of Adult and Continuing Education (NIACE) and the trade union movement through UnionLearn.
“Community Learning Champions are people who become active in their community by promoting the value of learning to others. They may be promoting learning with their friends, neighbours, relatives or workmates, but they could also be meeting people they meet meet at the school gates, at the local shops, or in groups or clubs. Champions speak from personal exerience and act as role models for learning. (from NIACE website)”
Legal capability for everyday life
This is Law for Life’s legal capability project which sets out to equip people to deal with law-related issues they are likely to encounter in the course of their lives. I came across it when I visited the excellent Community Links in Newham who are piloting it.
The project is run over six sessions and includes:
- Making sense of the law
- Getting help and finding out about the law
- Dealing with problems including practical skills
- Broader issues of influencing change and community engagement
Topics include Housing, Employment, Discrimination and Welfare Benefits.
What does this mean for local public health?
It is not sufficient for us to focus on health champions. Of course they have a tremendous contribution to make to democratising and improving local health services and we must continue to promote them.
However, if we are to make a real difference to the social determinants of health – we also have to get out of our silo (public health is meant to be cross sectoral after all!) and support work in other sectors that opens up access to similarly complex systems and two of the most important must be education and that concerned with access to justice.
This means that Health and Wellbeing Boards need to consider how to take a system level view of how citizens are supported in developing and using their experience and knowledge of key systems – health, education, legal – to ensure that people get access to the support they need, can take more control of their own lives and help shape local services to better reflect their priorities.
What do you think?
Am I alone in being a bit surprised how quiet the public health world is about Mid  Staffordshire Hospital NHS FT and the Francis report?
Staffordshire Hospital NHS FT and the Francis report?
I am not sure if this comparative silence is because Directors of Public Health have little responsibility here (see the Department of Health guidance for local government on the role of Directors of Public – Best Practice Guidance – issued in December 2012), or whether the profession is just breathing a collective sigh of relief because it is not under the media spotlight.
I think that public health has a crucial role to play here. Reading the Francis report I am clear about two things
- First – there was a culture of disrespect and appalling treatment to vulnerable people who expected the health service to care for them at a time when they were in great need.
- Second – that because of this treatment it is the case that some people died because this lack of care. However, it is unclear how many people did actually die. The report which is full of caveats and doubts presents a debate which walks around a figure of something between 400 to 1200 people over a period of 12 years. In other words between 33 and 100 people a year from April 1996 to March 2008 (Mid Staffordshire NHS FT Inquiry Vol 1 Section G Mortality Statistics Page 350 onwards). I really hope that I have understood this correctly – please feel free to correct me.
I do not want to diminish the awful experiences of people who had the misfortune ot be ‘cared for’ at Mid Staffs Hospital – but I am concerned that this focus on a poorly performing hospital and the next five that are in the pipeline diverts us from much wider failures in care and public health.
What concerns me is that there are much more significant examples of system failure – with a much greater incidence of preventable death and yet we accept them – there is no Francis Report to challenge these.
At a recent LGA Public Health Conference the excellent Chris Bentley gave a presentation on “Health and Wellbeing Boards with teeth – Interventions that Bite” . One of the challenges for Health and Wellbeing Boards is having a proper grip on the balance between need and actions to address these.
In his presentation he shared information from a study conducted by the University of Birmingham in 2006. The slide is below. We can see that in the UK there were 5.7m people who had CHD of whom the health system (I read this as primary care) was aware of only half and of these only 50% were compliant with their treatment. So of the total population of people with CHD only 20% were actually receiving and taking the treatment they needed! This is system failure on a massive scale – not in hospitals but in primary care in particular.

Of course it is worse than this – because there is a strong inequalities gradient to this picture and as Chris would be the first to say there is an even wider issue to do with societal inequalities such as poor quality housing, low income and lack of power.
As local authorities start to develop their leadership role with regard to the Health and Wellbeing of their communities it will be crucial that they take a balanced response to the challenges presented by Francis. This will mean a measured and thoughtful view on where the real system deficits are in their area and which are the ones that it is important to focus on. This view will affect the focus they place on relationships with the provider trusts, what they hope Healthwatch will achieve and most importantly the level of scrutiny they give to primary care provision and to work to address the social determinants of health.
It will be crucial that local public health provides a thoughtful and confident analysis that allows local politicians to get this balance right – otherwise we will end up being led by high profile, government led, media fuelled reports about priorities and not address much greater injustices locally.
Joining it up – Health Inequalities, Voluntary Sector Data and Citizens Advice Bureaux
Last year (Data, Health Inequalities and Localism) I wrote a piece on the potential that Voluntary Sector data has to help Health and Wellbeing Boards get a more rounded view of what is happening in their communities.
Since then there has been an increase in activity in this area – I want to focus on work that the Citizens Advice analytical team have led with support from the Department of Health.
All CAB use a standard data set. Citizens Advice has developed a template to capture this local data so that a bureau can provide a strategic picture on the social determinants of health to feed into of Joint Strategic Needs Assessments and Joint Health and Wellbeing Strategies. This begins to address a long standing concern of mine – that Bureau data is good at helping Citizens Advice make social policy arguments to government but has not been seen as a resource to help Bureaux provide local commissioners with information.
The template includes an introduction by Sir Michael Marmot (Institute of Health Equity). This provides a simple and clear explanation about the relevance of information and welfare rights services to actions that tackle heath inequalities.
The introduction itself is a useful advocacy tool to explain to sceptical public health professionals or members of Health and Wellbeing Boards why welfare rights and information services have a key role to play in tackling health inequalities. I have made it available here – Sir Michael Marmot Introduction.
Two of the Bureaux who have already used these templates to produce reports for their local health system are Shropshire and Wolverhampton.
The template report is structured into sections that show:
- Where people who use the CAB service live and the relationship this has to deprivation
- Responses to key social determinants of health such as Child Poverty, Fuel Poverty, Homelessness, Domestic Abuse, Environmental and Neighbour Problems.
- Vulnerable groups of people such as those with a disability and long term health problems.
The template report concludes with a short section on emerging needs. These are short reports – but they provide useful insights into need – here is an example looking at useage by people who live in the most deprived 20% of neighbourhoods.
Shropshire
In the case of Shropshire of the 9,009 people they saw in 2011/12 the 4 big issues were benefits and tax credits, debt, employment and housing.
The Shropshire CAB report Health and Poverty records that they saw 438 clients who lived in the 20% most deprived Super Output Areas. I reckon – multiplying this figure by 2.4 (to 1051) to allow for households (Source is ONS April 2012) this equates to approximately 12.5% of families living in those communities using the bureau. This calculation is based on the IMD for 2010 that states that there were 8,402 adults and children living in the most deprived quintile in Shropshire in 2010. So, 1051/8402)X100 = 12.5%.
The same approach could also be used when looking at issues such as Long Term Conditions and Disability.
Wolverhampton
The Wolverhampton CAB report The Health Impact of Good Advice uses the same basic template as Shropshire but contains much more detail. These are of course very different places – Wolverhampton is much more deprived and urban – Shropshire is a sparsely populated rural authority. Wolverhampton provided a service in 2010/11 to 10,357 people of whom 6,348 lived in the most deprived quintile. (IMD figures for 2010 show that almost 52% of Wolverhampton residents – 129,740 people – live in the most deprived quintile (population 249,500, 2011 census). Therefore Wolverhampton CAB saw roughly 12% of families living in the most deprived areas in the City.
My contention is that this level of connection – about 12% – with some of the most hard pressed families is impressive – these are small voluntary organisations who as well as providing a meaningful service are now able to provide information that goes some way to increasing the potential for a powerful local dialogue about:
- What is happening to some of the most vulnerable people in local authority areas
- Whether services are sufficient
- Which services are actually in contact with easily ignored communities and what potential there might be for extending the reach of other services through this.
If you are not impressed with this degree of contact – ask yourself the question – what proportion of these communities do public health programmes like smoking cessation, walking for health and healthy eating programmes etc reach?
A further step
Finally, Wolverhampton have taken this and other data and produced a short social policy report called Where to next, Poor city? This is a really helpful document starting to use the experience and insights from a comparatively small voluntary organisation to bring a thoughtful strategic social policy analysis to local commissioners.
Here is some information from ‘Where to next, poor city?’
- Housing Benefit cuts affect 4,000 households – there were 97,000 households in 2001
- 15,000 Disabled Claimants face re-assessment
- £80m is outstanding in County Court Judgements which will exlcude 1/3 of households from accessing normal high street credit.
- There are over 31,000 doorstep/pay day loans running
- In Wolverhampton 6% of local households recieve a monthly food parcel
This is a bleak but realistic picture. However, there is a real opportunity here. The trail blazing work by bureaux like Wolverhampton and Shropshire helps to contribute to a genuinely different discourse that focusses on the ‘causes of the causes’ and starts to help local authorities in particular champion their own public health priorities.
In Wolverhampton Jeremy Vanes the CAB Chief Executive talks about answering one question only – ‘how do we make every local household financially sustainable”?
What needs to happen
Local Commissioners should:
- Pro-actively engage with local CAB supporting and encouraging them to use their information.
- They should consider how they can put this information alongside information they hold to broaden and strengthen the analysis – particularly from a population perspective.
- They should consider how they can utilise the connectedness that local bureau have to work with CAB to build other health and wellbeing services around them and whether additional investment would help Bureau reach out to more people who are in greatest need.
What do you think?
Setting Priorities for Local Healthwatch
Setting Priorities for Local Healthwatch
As Local Healthwatch organisations start to be confirmed they will immediately feel pressure to demonstrate impact. What factors does local Healthwatch need to take into account when determining its priorities? I was asked to give a short talk (10 minutes!) at the Healthwatch England Conference held on the 6th of February in Leeds – this is what I said.
There are no quick answers to determining local priorities – but in determining priorities it may be helpful to consider the following:
Which areas of work to prioritise?
- Which tools are most important and when? – What is the right balance in terms of time and resources between Enter and View? data analysis? Service reviews? Which of these (and other tools) will make the biggest impact and under what circumstance?
- Information – what is the right balance between providing advice and information for the public and ensuring that advice and information is available across the local system?
- How much should local healthwatch be the consumer voice and how much should it ensure the consumer voice is heard?
- How much should the focus be on the way in which health and social care services are provided and/or on the type of services that are commissioned?
- Should local Healthwatch have a focus on treatment AND on prevention – what is the right balance?
- Issues to choose – the priority must be system and service level issues
Getting the right principles and values from the beginning
- Prioritise – the easily ignored, the vulnerable, people behind walls in institutions or isolated and lonely in their own homes.
- Inequalities
- People whose needs are difficult to meet or measure
- Does this lead us to mental health, learning disability, the vulnerable elderly, dementia?
Relationships – who to influence, work with and represent?
Its nice to be wanted but don’t be seduced by the invitations! Running from one meeting to the next!
- System Leaders. Which are the key system level relationships and do key leaders share the same ambition as local Healthwatch? Who are these people? Are they the leader of the local authority, cabinet lead for health, chair of health and wellbeing board, chair of CCG, chair of Overview and scrutiny are these the right people?.
- Citizens relationships – community development projects, community health champions, volunteers in community and big institutions like foundation trusts, area committees and partnerships – who is connected with active citizens?
- Structures – which are the most influential committees and which are the ones that you just need to know about – Health and Wellbeing Board, Local Quality Surveillance Groups, Overview and Scrutiny, Trust Boards, Voluntary Sector Partnerships, Special Interest Groups etc.
Data
Just because it is a statutory requirement does not mean that it is the best way of doing things!
- Joint Strategic Needs Assessment are important but bring a critical eye – they are often very physical health focussed and may not give enough attention mental health, social care, voluntary sector
- Other information is very important – but this will need building up into a credible framework and narrative – ICAS, Complaints about services, concerns raised at CABx and other welfare rights organisations, Patient Opinion, Feedback, Tribunals, Consultations – we need to know what information is available at a local level.
Impact
Quick Wins and the long term. Quick wins are important but local Healthwatch needs to have an informed view on long term challenges as well. These include:
- integration of health and social care,
- Social Determinants of Health,
- Funding for Adult Social Care,
- Prevention versus Treatment,
Opinions
The above are just a list of ideas and opinions not a definitive list – what do you think?
Public Health in Tough Times
 What should public health look like in tough times – what are the strategies and actions that will do the most to tackle health inequalities and support the most vulnerable?
What should public health look like in tough times – what are the strategies and actions that will do the most to tackle health inequalities and support the most vulnerable?
If you want to get a really good feeling for the scale of the challenge look at the latest publication from the Centre for Welfare Reform “A Fair Society? How the cuts target disabled people” this highlights that:
- Of the £75.2 billion to be cut by government by 2015 50% falls on two areas – benefits and local government – these two areas only make up 26.8% of government expenditure.
- Local Governments primary function (over 60%) is to provide social care to children and adults
- By 2015 local government and housing will be cut by £16.2 billion – a real terms cut of 41.9%
- Benefits for disabled people and the poorest will also have been cut by £18 billion a cut of about 20%
For comparison the Public Health budgets that will be passported over to Local Government for 2013/14 will be £2.6 billion and will rise slightly in 2014/5.
So the question for local government is what are the public health priorities now?
The local authority public health duties (what they can spend their ring fenced public health budgets on) are:
- improving significantly the health and wellbeing of local populations
- carry out heath protection functions delegated from the Secretary of State
- reduce health inequalities across the life course, including within hard to reach groups
- ensure the provision of population healthcare advice
Looking at the list I think that the economic and policy environment is such that as much of the budget has to be focussed on reducing health inequalities. Population based approaches are not a priority at the moment, health protection functions should be shared between local authorities and population healthcare advice can be paid by CCGs.
Working out what to do
In working out what actions to take it is important to watch out for dangerous diversions along the way. For example:
Demonisation – there is a real risk of falling into the paradigm that the coalition government is trying to create – treating the poor as ‘other’, as feckless. Jeremy Seabrook describes this consistent and dishonourable strand of our cultural history that goes back at least 500 years. It is dangerously easy to get sucked into promoting interventions that demonise the poor – as an extract from the recent LGIU/Westminster Council Report “A dose of localism the role of local government in public health” shows:
“Localisation of council tax benefit and housing benefit……provide an opportunity to embed financial incentives for behaviours that promote public health…When an exercise package is prescribed to a resident, housing and council tax benefit payments could be varied to reward or incentivise residents”
This proposal was summed up crisply by the Daily Mirror as ‘Overweight? Exercise or we’ll axe your benefits‘ I suppose it might feel better if high earners (senior civil servants, politicians, directors of public health?) were also told that unless they adopted healthy lifestyles they would have to pay more tax! Chance would be a fine thing.
Of course the proposal is unworkable anyway and not even very popular within the Conservative Party. See comments on the Conservative Home Blog
Disempowerment – the second diversion is disempowerment. Regulating the environment that poor people live in without giving them the chance to improve their circumstances. So we see Diane Abbots (Shadow Public Health Minister) recent proposal to allow local authorities to ban fast food joints from around schools. This approach can be traced back to the well intentioned paternalism of people like Titus Salt who built an alcohol free model village for his mill workers. My point is that knee jerk responses to regulate the environment that poor people live in are tokenistic unless they are part of a wider plan to provide positive alternatives.
Positive Actions
What is clear is that local authorities are already coming up with positive actions at a system level that address health inequalities and this is what public health budgets need to be supporting. It is also not suprising that many of these actions are consistent with the priorities (Housing, Income, Employment and Mental Health) that were captured in the Institute of Health Equity Report ‘The Impact of the economic downturn and policy changes on health inequalities in London’.
Some examples:
Poverty
- Blackpool Council has decided to provide a free breakfast and mid-morning drink of milk to all its 12,000 primary school pupils. This seeks to directly addresss one of the effects of poverty – poor diet. The intervention is universal and system level and there is an evidence base that gives the local authority confidence that the intervention will work.
- The Islington Fairness Commission is implementing a wide range of actions that include:
- Adopting the London Living Wage – and requiring all of its contractors to adhere to this too.
- Commissioning a new welfare rights service in the borough. In 2007/8 a survey commissioned by Age Concern (Just what the doctor ordered – welfare benefits and healthcare) estimated that for every £1 spent on welfare rights services £10 was put into the pocket of clients.
Housing
The London Borough of Newham have taken action to improve the quality of private rented housing bringing in a licensing scheme for all private landlords
Co-production
Finally a positive proposal from the LGIU/Westminster report. Which recognises the importance of co-production with citizens and developing assets in communities – models such as Turning Points Connected Care Model are being picked up by local authorities bringing communities, commissioners and providers together to delvier radical reform of services. A description of the Turning Point programme and other People Powered Health projects is available here
What do you think?
Doritos sponsors UK Faculty of Public Health Blog!
Well you have to give Doritos credit here. Hope they adhere to the latest salt guidelines!
Chief Medical Officer – Annual Report – Could do Better

Its worth having a look at the recent report by the Chief Medical Officer for England. The CMO is the ‘professional head of all Directors of Public Health’ and is working in an environment that is very similar to the one that local DsPH will soon be in – a senior officer advising politicians.
While this report (her first) has some strengths regrettably it largely fails to provide a positive example to DsPH about how to engage with and influence local decision makers.
Here are some of the challenges
The inspiration for this public health report is Sir John Simon – who was the second Chief Medical Officer from 1855 – 1876.
According to the UCLA website Simon was also first Medical Officer of Health for the City of London. In his first annual report in 1849 he called for municipal action to eradicate slums, build model dwellings for the poor, provide public wash-houses, take control of the water supply, suppress offensive trades, provide a municipal cemetery, complete the drainage system, and establish a permanent sanitary inspector. The website tells us that he used his considerable political influencing skills to achieve these changes – precisely the skills required by local DsPH and the CMO.
Regrettably this report does not convince that his legacy continues.
With its list of over 50 medical conditions this is a return to a style of public health reporting that local public health leaders have increasingly tried to get away from as they have sought to give clear messages about priorities and actions that will engage, motivate and energise none health sectors and organisations that can make the biggest difference to health and wellbeing.
This is a shame because hidden away within it are concerning figures that should form the basis of an assertive call to action.
Page 245 – Healthy Standard of Living – Percentage of children living in poverty
Page 246 – Percentage of Households in Fuel Poverty
These figures show respectively a failure to reduce levels of poverty and a worrying increase in the number of households in fuel poverty.
Some of the solutions here rest with government – and require more than pious calls ‘for local authorities to actively promote the uptake of insulation’
Mental Health
The Governments Mental Health Strategy notes that this is the first government to give an equal weighting in policy terms to mental and physical health – regrettably this is not the case with regard to this report. In 300 pages there are 4 are devoted to mental health.
According to this report an estimated 6.1m people suffer from anxiety and depression in England. While it notes that currently just over 2% currently get access to IAPT services it draws no link between the relationship between housing insecurity, financial vulnerability and poor mental health.
This is a serious omission; by focussing on individual illnesses and diseases the CMO does not make a consistently strong link with ‘the causes of the causes’
Peoples social and economic circumstances affect their mental health and wellbeing. If people feel good about themselves and in control then they are more likely to be able to live healthily.
In presenting lists of data with no apparent order to them the report fails to give a clear message about where we should start from; particularly wth regard to the prevention agenda, and fails to empower local DsPH and Local Authority Cabinet Leads for Health with clear messages about pratice. She repeats the same mistake that JSNAs have been criticised for locally – lots of data and no clear view about priorities.
It is disapointing to include reference to the life course on pages 14 and 15 of the document and then to structure the report as a series of lists that ignores this framework.
No Assets
The report is a long list of deficits. At a local level many Directors of Public Health are seeking to develop a narrative that balances a description of need with the assets that exist in local communities. The CMO is in a unique position to provide a complementary view at a national level – and fails to do so.
With privileged access to cross government information on housing, volunteer involvement, investment in the voluntary and community sector, and with the Departments own Voluntary Sector Strategic Partner Programme to call on this would have been the place to show leadership and mandate innovation at a local level. None of this is referenced in the report.
Recommendations
I will comment on two of them.
Recommendation 2 – Physical Health and Mental Health and Wellbeing
The call for better data on resilience and wellbeing should go some way to addressing some of the deficits I have highlighted earlier with regard to mental health. To be frank this is urgent. The NHS is still driven by a narrow view of evidence based commissioning. If data does not exist then commissioners will continue to focus on areas where they can collect data – and as this report demonstrates that is predominantly siloed data about physical health conditions.
However, this recommendation calls for data being available at a national level. What the CMO needs to understand is that most commissioning now happens locally. She needs to be urging government agencies such as ONS, DH and other Government Departments to prioritise making information available to local authorities and CCGs that will help them commission more effectively to meet the needs of their populations.
Recommendation 4 Social Determinants
Frankly I struggle to follow this. The CMO highlights the challenges here – low income, poverty, lack of access to education and training and her recommendation is…….build on the olympic legacy!
I find this staggering. At a time of economic crisis and government policies that impact particularly negatively on the poorest and most disadvantaged the key solution is to maximise the legacy of the Olympics!
As local authorities face the biggest cuts they have ever experienced I think this will be met with hollow laughter – talk about sending your Director of Public Health naked into the Health and Wellbeing Board!
Conclusion
Regrettably this report fails to recognise the challenges that local Directors of Public Health face, does not respond to the localist agenda and does not sufficiently reflect the developments in public health thinking with regard to the Marmot framework, co-production, assets and citizens voice.
What do you think?
Good Riddance! Government Abolishes Public Health Cabinet Sub-Committee

Who cares?
In the public health world there has been a bit of outrage over the governments decision to abolish the cabinet sub committee on public health (see page 8 of this report for its original membership and remit). I realise this will seem a bit parochial to those of you not in the ‘public health family’, but hear me out.
The Cabinet Public Health Sub Committee was announced in Healthy Lives, Healthy People: Our strategy for public health in England as the means by which the Secretary of State would ‘lead public health across central government’ (para 4.56) and ‘work across multiple departments to address the wider determinants of health’ (para 3.4).
The reason given for its abolition is that other government departments were not turning up to the meetings so there was little point it continuing to exist.
I am in a bit of a quandary here. Cabinet Sub Committee papers are not publicly available – so I have no idea what was discussed, who attended (or did not attend) and what difference this meeting made.
Evidence
I struggle to see the difference it has made. Lets look at some wider policy areas that impact on the health and health inequalities. For a good up to date summary of the evidence see this recent report from the Institute of Health Equity.
- Welfare Reform Policy – does not seem to have taken into account the impact on the health and wellbeing on some of the most vulnerable – I have no idea if the Cabinet Sub-Committee on Public Health has discussed welfare reform. If it has what difference have the discussions made to the implementation of Employment Support Allowance, the Housing Benefit Cap etc?
- Abolition of Education Maintenance Allowance – Was this discussed at the cabinet sub-committee on public health and how did this discussion affect implementation of this policy.
- Funding support for early interventions – Government changes to business rates and early intervention grants are likely to lead to significant further reductions to SureStart services.
What should the public health profession do?
I am no supporter of this government or its policies but at the end of the day it was the responsibility of public health leaders to ensure that this sub-committee made a useful contribution and I think they failed. This despite a policy environment that actually presents a range of potentially useful levers – the work of the Institute for Health Equity makes a powerful case for a Health in All Policies Approach and the Department for Health does listen to them; the transition of public health to local government strengthens the potential for collaboration with the Department for Communities and Local Government; the growth in ideas around Citizenship and the Big Society still has interest at the top of Government; and of course there is the Public Health Responsibility Deal – that should connect with the Department for Business, Innovation and Skills.
Now, just because I mention the little list of policy levers above – don’t think that I am endorsing or supporting all of them. My point is that in the world of realpolitik there were plenty of pegs to hang a meaningful agenda for a cross cutting government committee – and yet public health failed to capitalise on this.
Do we care………really?
In my view the abolition of the Public Health Subcommittee is a blessing. Because in addition to the two reasons I mention above – lack of accountability and impact – its a diversion!
The real game is a local one. The public health profession in England needs to work within the national policy environment through local authorities to improve health and reduce health inequalities. Of course this means sometimes working in a context where government policy will be working against local health and wellbeing and worsening health inequalities. The public health task is to empower local politicians (Councillors and MPs) to make this clear to national government – they should be leading this debate and we should be supporting them.
A secret committee to improve wellbeing!
While having a cabinet sub-committee on public health is flattering and seductive it risks incorporation. The idea that a secret unaccountable committee is somehow an essential part of effective policy making at a national level is patently nonsense. It is even more outrageous when we consider that public health is about people taking control of their health and wellbeing. Do we really need a secret government committee to consider this?
Lets face it In the post Lansley world the role of the Department of Health is considerably reduced. The real action is going to be taking place in Public Health England, Local Government, the Voluntary and Community Sector and Clinical Commissioning Groups.
We need to focus on strengthening our local accountability and building our local base and make sure that future engagement with the government is in public and wherever possible through locally elected leaders – in the long term this might be more effective.
What do you think?
Who Cares about the Department of Health Responsibility Deal?
My instinctive reaction to the Responsibility Deal brought in by Andrew Lansley was to be against it – believing it to be window dressing to cover up the fact that the Department of Health had little intention of using legislative and policy muscle to force the private sector to damage health less and promote it more.
to be against it – believing it to be window dressing to cover up the fact that the Department of Health had little intention of using legislative and policy muscle to force the private sector to damage health less and promote it more.
I have nothing against collaborations with private sector organisations, those of us who work at a local level know that local authorities and other local statutory bodies cannot legislate. They rely on influence, negotiation and collaboration to achieve change. Structures like Local Strategic Partnerships were examples of attempts to achieve strategic collaborations for the good of communities – and Health and Wellbeing Boards will have similar ambitions.
I am also not in favour of creating laws to achieve change if this can be achieved through other means. So it is important to judge the Responsibility Deal on its own terms – on what it has achieved.
Three ways to assess the Responsibility Deal.
- Strategic – focussed on priority areas
- System level impact
- Accountable to the public
Strategic Focus
The Responsibility Deal focusses on the following areas.
Alcohol – primarily about information and also trying to increase the availablity of lower alochol drinks.
Food – primarily about information, reducing salt, reducing transfats, availablity of lower calorie and healthier food.
Health at Work – primarily about supporting those with chronic conditions to stay in employment, quality of occupational health services, accountability for sickness levels, food for staff, stop smoking services, staff health checks, mental heath workplace adjustments
Physical Activity – enabling phsyical activity in communities, promoting active travel, increasing physical activity in the workplace, tackling barriers to participation by the most inactive.
These areas bear little relation to the more coherent model proposed by Duncan Selbie Head of Public Health England which I referenced in an earlier post.
| % Impact on Health | Policy Area | Examples of relevant sectors |
| 40 | Social and Economic | Banking, Finance and Employment |
| 30 | Health Behaviours | Food and Alcohol |
| 20 | Clinical | Health |
| 10 | Environmental | Transport and Housing |
As the above table shows the Responsibility Deal is focussed almost exclusively on Health Behaviours – aside from a small amount of activity on workplace health, it largely ignores the areas that have the greatest impact on health.
Impact
Ownership
The most recent update (July 2012) tells us that there are 390 partners – I reckon this probably now stands at about 450. This means that the responsibility deal has been gathering partners at a rate of approximately 6 a week – I don’t know if this is good or not.
The update also notes that 75% are private sector organisations. So just under 300 are from the private sector.
According to the governments own statistics there are 4.5m enterprises who employ over 23m people; of these 99.2% are small enterprises employing less than 49 employees. 6,320 employ more than 250 employees; 30,475 employ between 50 – 249.
It is clear that the Responsibility Deal has barely scratched the surface in terms of connecting with the private sector.
Where it does better is when it is working in environments that are dominated by very few companies – such as food retail where the ‘big 4’ control about 75% of the market.
I have already indicated that it is very hard to understand the degree of impact because the way in which the information is presented means that it is not possible to get a feeling for the system level impact of the various pledges.
Outputs
The Responsibility deal has got some traction – for example the Food and Drink Federation Annual Review for 2011 which was published in April 2012 devotes a page to the deal and they have also supported production of the Workplace Wellbeing Toolkit – which has an introduction by Dame Carol Black.
Outcomes
This is where I really start to struggle. For example in July 2012 Dr Susan Jebb who is chair of the food network states that “the average amount of salt we’re eating in England has declined by .5g a day between 2008 and 2011. It shows clearly that the huge effort by the food industry to reformulate products to reduce salt is paying off”. I’ve no problem with any of that – except that the time period and all these gains were made before the Responsibility Deal was even established!
I suspect that many companies who have a high public profile were already very involved in this agenda well before the Responsibility Deal – for example Tesco tell us that since 2006 they have removed 3,000 tonnes of salt from their range.
It does claim to have made progress in areas such as providing information to the public through labelling – but I am unclear how much additional progress has actually been caused by the Responsibility Deal itself.
There are 27 responsibility deal pledges in total some of the more popular ones – particular around alcohol and food can have 80 or more signatories signing up and committing to report.
Weaker pledges where sign up and commitment to report is poor include:
- Awareness of alcohol units off and on trades – just over 40 companies
- Alcohol Unit Reduction – just over 30 companies
- Calorie Reduction – 21 companies
- Salt Reduction Training and Kitchen Practice (Catering) 8 companies
- Salt Catering – reformulation of products – 7
- Smoking Cessation – 26 of which 14 are not for profit organisations
- Staff Health Checks – 34 of which 15 are not for profits
- Mental Health workplace adjustments – 5 of which 2 are not for profits
- Physical Activity Inclusion – 54 of which 24 are not for profits
Frankly some of these figures are damning. Particularly those on mental health workplace adjustments. These are measures of corporate irresponsibility – or the irrelevance of the initiative or pledges.
Accountability
Page 6 of the launch document states that
“monitoring progress is key to establishing accountability by confirming the actions that organisations have pledged to take have been completed. Similarly evaluation has an important role to play in showing the public and other interested parties, as well as the partners themselves the impact of the Deal in changing behaviours and improving health outcomes.”
I can’t disagree with any of the above. The problem is that the way the information is presented and the spin that is put on it means that it is not possible to meet this ambition.
The June 2012 update states that “the Responsibility Deal has moved further and faster than could have been achieved through the regulatory route”. I can see no evidence for this. For example the update tells us that 47 partners have signed up to provide simple and consistent information for the On Trade and that together they control 19,500 premises – sounds impressive – however, there are almost 120,000 licensed on trade premises in England and Wales – I am not convinced that signing up about a quarter of companies is moving “further and faster.”
Unfortunately the way the data is presented – non contextualised information; individual company information in separate spreadsheets and little aggregated data means that it is not possible to make a judgement about impact and performance
Lessons
Positives
- Some key industry bodies do seem to have bought in to the Responsibility Deal
- Many major companies do seem to be members
- Some useful tools have been produced by the industry
- There is the potential for dialogue with industry
Negatives
- Many high profile companies were already engaged in this work before the Responsibility Deal was created and the added value is unconvincing
- The number of organisations involved is very small
- The degree of buy in on important but difficult areas such as mental health at work, staff health checks and inclusion is embarrasingly poor
- It is very hard to hold the Responsibilty Deal partners and the Department of Health to account because information is presented in such a poor way and when summarised it is often ‘spun’ to give as positive picture as possible.
- The focus is not strategic – with an emphasis on food and alcohol. There is a failure to engage wider sectors such as finance or housing – to encourage them to take action to improve health
What do you think?
